Emerging therapies for heart failure with preserved ejection fraction

Heart failure
Despite significant advances in treatment for both coronary artery disease and systolic heart failure, there are no therapies that have yet been developed to reduce mortality or to consistently relieve symptoms in patients with heart failure with preserved ejection fraction.
- Heart failure with preserved ejection fraction (HFpEF) is projected to become more prevalent than heart failure with reduced ejection fraction (HFrEF) over the coming years.
- Exercise stress assessment of diastolic function, particularly by right heart catheterisation, is emerging as the gold standard test in the diagnosis of HFpEF. Right heart catheterisation can confirm the diagnosis and also assist in dose-titration of diuretic and other medical therapy.
- Current evidence-based therapies for heart failure with reduced ejection fraction have been trialled in patients HFpEF with limited success.
- Promising novel treatments include newer pharmacological therapy and inter-atrial shunt device implantation.
- Current management is focused on lifestyle modification (weight loss and exercise), blood pressure control, judicious use of diuretics to maintain fluid balance and management of comorbidities such as atrial fibrillation. Presently, prescribed exercise training and weight loss are the most effective disease-modifying therapies.
Picture credit: © Scott Bodell/Medical Images
Heart failure is the leading cause of hospital admission in adults aged over the age of 65 years. Heart failure with preserved ejection fraction (HFpEF, previously called diastolic heart failure) is as common as heart failure with reduced ejection fraction (HFrEF, systolic heart failure) and is projected to become more prevalent within the next few years.1,2 Despite the development of significant advances in drug and device therapy for both coronary artery disease and heart failure with reduced ejection fraction, there are no therapies that have yet been developed to reduce mortality in patients with HFpEF or to consistently relieve symptoms.3
A classic patient with HFpEF is female, overweight and has a history of hypertension; however, multiple phenotypes exist. The presentation is progressive exertional dyspnoea in the absence of obvious contributing comorbidity, and patients have normal systolic function on transthoracic echocardiography. Confirming the diagnosis is essential, not only for the patient and clinical team to understand the cause of symptoms and to offer appropriate therapies for symptom relief but also to offer the patient trials of novel emerging therapies.
Advances in diagnosis
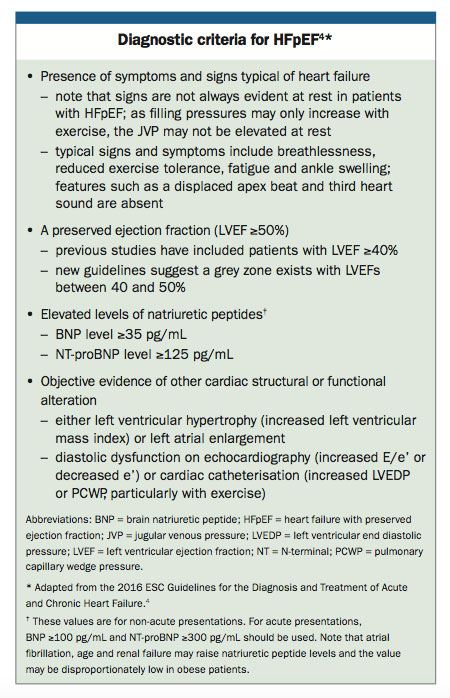
The mechanistic understanding of HFpEF has grown over the past decade, with increased understanding of the various patient subtypes and underlying pathological mechanisms, suggesting physiological targets for therapy. The diagnostic criteria for HFpEF have changed, with more stringent echocardiographic criteria (summarised in the Box).4
{kind=link}
Right heart catheterisation
As symptoms and physiological abnormalities are often not present at rest, exercise stress assessment of diastolic function, particularly by right heart catheterisation, is emerging as the gold standard test in the diagnosis of HFpEF.5 Right heart catheterisation can provide direct confirmation of elevated filling pressures during exercise testing and assist in dose-titration of diuretic and other medical therapy.
In centres where a high volume of these catheterisations are performed, the procedural risk is low and it is increasingly being performed through a brachial venous approach to enhance patient comfort and reduce recovery time.6 In our centre, catheterisation is performed predominantly through a cubital venous approach and exercise is undertaken using supine cycle ergometry. The patient is discharged one hour after completion of the procedure.
Existing therapies
Current evidence based therapies for heart failure with reduced ejection fraction have been trialled in HFpEF with limited success. Large randomised trials of using angiotensin converting enzyme (ACE) inhibitors and angiotensin receptor blockers have not demonstrated positive primary outcomes. In a large multicentre trial, spironolactone use was associated with reduced hospitalisation for heart failure but also with higher rates of hyperkalaemia and renal dysfunction.7
Beta blockers have been hypothesised to prolong diastolic filling time but results have been conflicting because they must be used cautiously in the subgroup of patients with chronotropic incompetence (inadequate increase in heart rate to meet increase in activity or demand).8,9 Use of the combination agent sacubitril–valsartan, a neprilysin-angiotensin receptor inhibitor, has been shown to significantly reduced mortality in patients with heart failure with reduced ejection fraction, and early data suggest a positive outcome in patients with HFpEF.10
The disappointing outcomes of large trials of neurohormonal agents in treating patients with HFpEF are due in part to the heterogeneity of the patient populations studied. Cluster analysis based on a combination of clinical and echocardiographic variables has identified homogenous subgroups, and the subsequently postulated theory is that matching specific heart failure therapies based on both clinical and physiological phenotype will improve outcomes.11
Emerging therapies
Therapies targeted at underlying physiological abnormalities are the key to the successful treatment of HFpEF, and multiple pharmacological targets are currently under investigation.12
Medical therapies
Trials of blood pressure control in hypertensive patients with HFpEF have shown fewer heart failure events; this underlines the importance of risk factor management.13,14
Recent studies focusing on the role of modulation of the nitric oxide and soluble guanylate cyclase pathways have produced mixed results.15,16 A randomised trial of isosorbide mononitrate demonstrated adverse effects on patient activity levels; similarly, the results with vericiguat (a soluble guanylate cyclase stimulator) in a recent large randomised trial were disappointing from a physical and biochemical perspective, although they suggested small improvements in quality of life.17 A small scale study addressing the role of phosphodiesterase type III inhibition with intravenous milrinone has shown potential for use in patients with HFpEF.18 Further studies are assessing the roles of inhaled nitrite, ivabradine, ranolazine and iron replacement therapy.
Surgical therapy
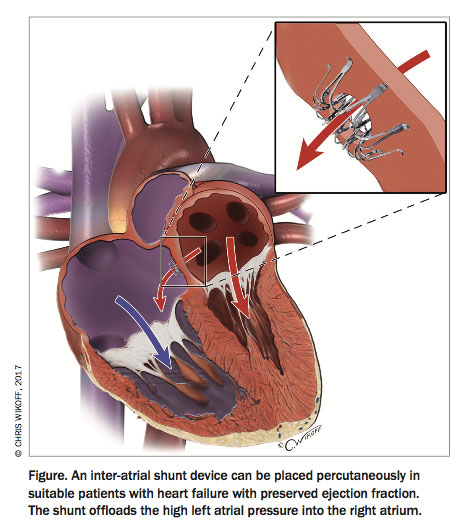
Newer developments in therapy include a novel inter-atrial shunt device, which is placed percutaneously during cardiac catheterisation. This creates an 8 mm diameter shunt between the atria, allowing the high left atrial pressures seen in HFpEF to be offloaded into the right atrium, with improvements in pulmonary pressures and functional capacity (Figure).19,20
{kind=link}
Further trials are being conducted to assess the benefits of renal denervation, atrial pacing, elastic expansion devices and baroreflex modulation.21
Lifestyle modification
Lifestyle modification is essential in patients with heart failure.22 Exercise training and weight loss have produced strongly positive effects in patients with HFpEF – this is the most effective disease-modifying therapy at present.23
Exercise has both central and peripheral effects, and the benefits extend across the age spectrum – although the specific physiological effects may differ. The use of specific guidelines for exercise training in heart failure and endurance training has been associated with improvements in function and quality of life in small studies.24
Weight loss reduces inflammation, improves endothelial function and has a direct effect on diastolic function. Similarly, treatment of comorbidities may have a large impact in patients with HFpEF; often hypertension, atrial fibrillation, obesity, iron deficiency, coronary disease and respiratory disease are present.25–28
Conclusion
The endpoint in major cardiovascular trials has usually been a reduction in mortality. HFpEF is predominantly a syndrome of the elderly, and its effect on quality of life and functional capacity is profound. In addition to mortality and hospitalisation, future trials should focus on functional capacity and quality of life, and it has been suggested that these parameters be included in regulatory pathways for drug approval.29
The therapeutic landscape in HFpEF has been limited, predominantly due to poor specificity in definition, a limited mechanistic understanding of the condition and heterogeneity within the patient population. The past five years have yielded significant insights into the physiological mechanisms underpinning the disease. Improved recognition by primary care physicians and shared care with centres experienced in the management of and having dedicated clinics for treating patients with HFpEF will lead to improved outcomes.
Despite the unsatisfactory outcomes in regard to disease modifying therapy in HFpEF, clarity around diagnosis is critical to ensure symptom relief through adequate optimisation of fluid balance. Current management is focused on lifestyle modification (weight loss and exercise), blood pressure control, judicious use of diuretics to maintain fluid balance and management of comorbidities, such as atrial fibrillation. Echocardiography and exercise right heart catheterisation can confirm the diagnosis and guide therapy for symptom relief.30 Dedicated specialised HFpEF clinics, designed to combine investigations and management approaches with early access to research trials, may improve the management of this complex and common condition.
References
- Chan Y, Gerber T, Tuttle C, et al. Rediscovering heart failure: the contemporary burden and profile of heart failure. Melbourne: Mary MacKillop Institute for Health Research; 2015.
- Oktay AA, Rich JD, Shah SJ. The emerging epidemic of heart failure with preserved ejection fraction. Curr Heart Fail Rep 2013; 10: 401-410.
- Nanayakkara S, Kaye DM. Management of heart failure with preserved ejection fraction: a review. Clin Ther 2015; 37: 2186-2198.
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2016; ehw128.
- Borlaug BA, Nishimura RA, Sorajja P, Lam CS, Redfield MM. Exercise hemodynamics enhance diagnosis of early heart failure with preserved ejection fraction. Circ Hear Fail 2010; 3: 588-595.
- Khera R, Pandey A, Kumar N, et al. Variation in hospital use and outcomes associated with pulmonary artery catheterization in heart failure in the United States. Circ Heart Fail 2016; 9: e003226. Available online at:
- http://circheartfailure.ahajournals.org/content/circhf/9/11/e003226.full.pdf?download=true (accessed June 2017).
- Pitt B, Pfeffer MA, Assmann SF, et al. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med 2014; 370: 1383-1392.
- El-Refai M, Peterson EL, Wells K, et al. Comparison of beta-blocker effectiveness in heart failure patients with preserved ejection fraction versus those with reduced ejection fraction. J Card Fail 2013; 19: 73-79.
- Edelmann F, Musial-Bright L, Gelbrich G, et al. Tolerability and feasibility of beta-blocker titration in HFpEF versus HFrEF: Insights from the CIBIS-ELD trial. JACC Heart Fail 2016; 4: 140-149.
- McMurray JJ, Packer M, Desai AS, et al. Angiotensin–neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014; 371: 993-1004.
- Solomon SD, Zile MR, Pieske BM, et al. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet 2012; 380: 1387-1395.
- Shah SJ, Kitzman DW, Borlaug BA, et al. Phenotype-specific treatment of heart failure with preserved ejection fraction. Circulation 2016; 134: 73-90.
- Edelmann F, Wachter R, Schmidt AG, et al. Effect of spironolactone on diastolic function and exercise capacity in patients with heart failure with preserved ejection fraction: the Aldo-DHF randomized controlled trial. JAMA 2013; 309: 781-791.
- Cleland JGF, Tendera M, Adamus J, Freemantle N, Polonski L, Taylor J. The perindopril in elderly people with chronic heart failure (PEP-CHF) study. Eur Heart J 2006; 27: 2338-2345.
- Hasenfuß G, Hayward C, Burkhoff D, et al. A transcatheter intracardiac shunt device for heart failure with preserved ejection fraction (REDUCE LAP-HF): a multicentre, open-label, single-arm, phase 1 trial. Lancet 2016; 387: 1298-1304.
- Feldman T, Komtebedde J, Burkhoff D, et al. Transcatheter interatrial shunt device for the treatment of heart failure. Circ Hear Fail 2016; 9: e003025.
- Zamani P, Rawat D, Shiva-Kumar P, et al. Effect of inorganic nitrate on exercise capacity in heart failure with preserved ejection fraction. Circulation 2014; 131: 371-380.
- Bonderman D, Pretsch I, Steringer-Mascherbauer R, et al. Acute hemodynamic effects of riociguat in patients with pulmonary hypertension associated with diastolic heart failure (DILATE-1): a randomized, double-blind, placebo-controlled, single-dose study. Chest 2014; 146: 1274-1285.
- Kaye DM, Nanayakkara S, Vizi D, Byrne M, Mariani JA. Effects of milrinone on rest and exercise hemodynamics in heart failure with preserved ejection fraction. J Am Coll Cardiol 2016; 67: 2554-2556.
- Patel HC, Rosen SD, Hayward C, et al. Renal denervation in heart failure with preserved ejection fraction (RDT-PEF): a randomized controlled trial. Eur J Heart Fail 2016; 18: 703-712.
- Kass DA, Kitzman DW, Alvarez GE. The restoration of chronotropic competence in heart failure patients with normal ejection fraction (RESET) study: rationale and design. J Card Fail 2010; 16: 17-24.
- Georgakopoulos D, Little WC, Abraham WT, Weaver FA, Zile MR. Chronic baroreflex activation: a potential therapeutic approach to heart failure with preserved ejection fraction. J Card Fail 2011; 17: 167-178.
- National Heart Foundation of Australia (NHF) and the Cardiac Society of Australia and New Zealand (Chronic Heart Failure Expert Writing Panel). Guidelines for the prevention, detection and management of chronic heart failure in Australia. 2011.
- Pandey A, Parashar A, Kumbhani DJ, et al. Exercise training in patients with heart failure and preserved ejection fraction: meta-analysis of randomized control trials. Circ Heart Fail 2014; 8: 33-40.
- Haykowsky MJ, Brubaker PH, Stewart KP, Morgan TM, Eggebeen J, Kitzman DW. Effect of endurance training on the determinants of peak exercise oxygen consumption in elderly patients with stable compensated heart failure and preserved ejection fraction. J Am Coll Cardiol 2012; 60: 120-128.
- Paulus WJ, Tschöpe C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol 2013; 62: 263-271.
- Edelmann F, Stahrenberg R, Gelbrich G, et al. Contribution of comorbidities to functional impairment is higher in heart failure with preserved than with reduced ejection fraction. Clin Res Cardiol 2011; 100: 755-764.
- Patel RB, Vaduganathan M, Shah SJ, Butler J. Atrial fibrillation in heart failure with preserved ejection fraction: insights into mechanisms and therapeutics. Pharmacol Ther 2016: doi: 10.1016/j.pharmthera.2016.10.019. [Epub ahead of print].
- Butler J, Hamo CE, Udelson JE, et al. Exploring new endpoints for patients with heart failure with preserved ejection fraction. Circ Heart Fail 2016; 9: e003358.
- Nanayakkara S, Mariani JA, Kaye DM. Heart failure with preserved ejection fraction: improving diagnosis and management. Med Today 2017; 18(1): 37-42.