Asthma, COPD and when they coexist

Asthma
COPD (chronic obstructive pulmonary disease)
Asthma and chronic obstructive pulmonary disease (COPD) are complex and heterogeneous inflammatory diseases of the airways. This review examines the impact that recent advances in our understanding of these diseases are having on the way we manage these disorders.
- Asthma and chronic pulmonary obstructive disease (COPD) are umbrella terms that describe disorders of the airways with diverse inflammatory pathways and pathophysiology.
- Recent advances in the understanding of the immunopathology of asthma have led to the emergence of biological agents that more precisely target disease pathways, but will require a more precise understanding of those dysfunctional pathways.
- There are areas where the pathology and expression of airways disease in asthma and COPD overlap.
- The overlap between asthma and COPD presents important challenges in diagnosis as well as management.
Picture credit: © Denkou Images/Diomedia.com
Asthma and chronic obstructive pulmonary disease (COPD) have, in reality, always been umbrella terms. Although both disorders occur largely in the bronchial airways, asthma is a major condition of childhood and adolescence whereas COPD is limited to adults. It has never been asserted that either condition results from a single pathology with predictable course and treatment. In fact, for the diseases that we now call asthma and COPD, the clinical diagnosis essentially relies upon definitions from 50 or more years ago.
How we have come to define COPD and asthma
The key clinical symptoms of asthma have been reported since ancient times and are little changed from Salter’s description in the 19th century of ‘paroxysmal dyspnoea of a peculiar character with intervals of healthy respiration between attacks’. Similarly, the definition and description of chronic bronchitis are little changed today from 1837, when Stokes described ‘inflammation of the mucous membrane’ in autopsy specimens. Similarly, emphysema was first recognised as a unique entity by Laennec in 1821, as a disorder of the alveoli and hyperinflation with gas trapping – defined by pathology, not aetiology or symptoms.
Advances in respiratory physiology in the 1950s and 1960s saw asthma and COPD recognised as disorders causing airflow limitation and provided a clinical test that could confirm and distinguish the diagnoses.1 The American Thoracic Society defined chronic bronchitis in clinical terms – chronic cough lasting at least three months per year for at least two years. Emphysema was primarily described in anatomical terms – enlarged alveolar spaces and loss of alveolar walls. On the other hand, asthma was described as a state of airway hyper-reactivity to a variety of stimuli. Asthmatic bronchitis was then considered an overlapping condition.1
Chronic bronchitis and emphysema were first grouped together under the term COPD in 1965 as both were reaching epidemic proportions and often coexisted. It was acknowledged that heterogeneity of processes could occur, but both were overwhelmingly being caused by cigarette smoking, which had increased following World Wars I and II.2
Heterogeneity in asthma
In the 1980s, it became clear that airway inflammation played a crucial role in asthma – it was not just a disorder of hyper-reactive airways. This was deduced from the positive effect that treatment with low-dose inhaled corticosteroids (ICS) had on improving outcomes for most patients with asthma.3 At the same time, advances in immunology and the development of sophisticated in vivo models of asthma led to an improved understanding of asthma and also a greater appreciation of heterogeneity within the condition.4
Clinical heterogeneity
Heterogeneity in asthma has been recognised for some time and was initially based on different patterns according to the main trigger. It was described as extrinsic asthma when the trigger was allergen exposure and intrinsic asthma when the triggers were not defined but there were maladaptive airway responses. This approach was soon found wanting, particularly in light of the efficacy of ICS in modifying the disease process in both groups and the overlap in the biology.5
The value of ICS in modifying the disease process in most people with asthma has now led to studies that better define the importance and the nature of airway inflammation in asthma. This has also supported the concept that if we could target treatment to suppress this inflammation we could improve outcomes further.5
Pathological heterogeneity
More recently, the use of induced sputum from patients with asthma has allowed assessment of the airway biology. Subsequently, variable patterns of airway inflammation have been described: elevated eosinophils, elevated neutrophils or paucigranulocytic (having neither of these granulocytes).6 This also led to the first attempts to define endotypes in asthma that may respond to targeted therapy. An endotype is a subtype of a condition defined by a specific biological mechanism. Airway eosinophilia has been shown to predict a favourable response to corticosteroid treatment, in contrast to a neutrophilic or paucigranulocytic pattern.7,8
Molecular phenotyping
A more detailed, molecular phenotyping approach has been taken using bronchoscopic epithelial brushings from steroid-naïve patients with mild asthma.9 Researchers have concluded that patients with asthma can be differentiated as having either high or low expression of epithelial cell gene signatures for the activity of T helper-2 (TH-2) cytokines.9 They found a correlation between airway eosinophilia and TH-2 gene expression, which may then be an indicator of corticosteroid responsiveness.10
The airway epithelium and the interaction with the innate immune response also appear to drive TH-2 inflammation and may explain inflammation in the absence of allergy sensitisation.11 For asthma refractory to ICS, monoclonal antibodies targeting the maladaptive immune responses are being used to individualise treatment.12 Monoclonal antibodies can be highly effective in a subset of patients with persisting abnormalities; therefore, greater accuracy using biomarkers of pathology and disease activity is needed when managing patients with refractory asthma.
Disease phenotypes
There is now a strong move to recognise heterogeneity in asthma by describing disease phenotypes, classifying patients into distinct subgroups. Currently, this classification depends on the patient’s history, prognosis and response to therapy. This approach is intended to help target treatment more effectively, although research is still needed on defining different treatments for different phenotypes. Emerging results have suggested several relevant asthma phenotypes (Table 1).4
Heterogeneity in COPD
The pathology of COPD is well described with a spectrum of disease that includes chronic mucus hypersecretion, goblet cell hyperplasia and small airway remodelling with loss of bronchioles and alveolar structures.13 As in asthma, infiltration with mixed inflammatory cells in the airways is the rule, but less is known about the role of these cells in COPD, the pathways causing disease and progression, and why treatment with corticosteroids is not effective. There also appears to be a greater degree of tissue remodelling and loss of peripheral airways in COPD.14
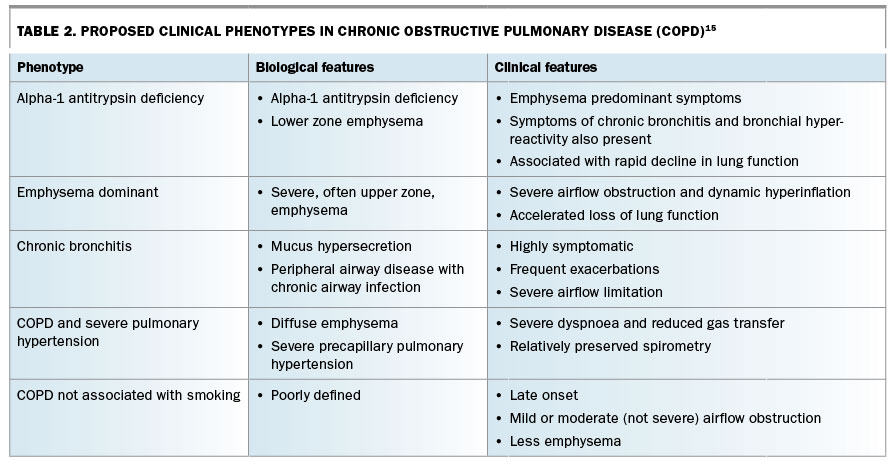
The clinical heterogeneity of COPD is well recognised and has grown with advances in biology and clinical imaging. Some of these phenotypes have recently been summarised and, as in asthma, they include groupings that are recognisable to clinicians (Table 2).15 Conspicuously absent from this list are those with the recently-coined term of asthma–COPD overlap syndrome (ACOS), which is discussed below.15
{kind=link}
Unearthing asthma–COPD overlap syndrome (ACOS)
Distinct guidelines for asthma and COPD
National and international guidelines for both asthma and COPD have been acknowledged as playing an important role in standardising diagnosis and recommending practical treatments for healthcare professionals. The recent Global Initiative for Asthma (GINA) now states that asthma is: ‘a heterogeneous disease, usually characterised by chronic airway inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation’.16
The most widely accepted definition of COPD comes from the Global Initiative for Chronic Obstructive Lung Disease (GOLD).17 COPD is described as ‘a common preventable and treatable disease, characterised by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lungs to noxious particles or gases’.17 Diagnosing COPD relies on objective demonstration of airflow obstruction that is not fully reversible, with a ratio of forced expiratory volume in 1 second (FEV1 ) to forced vital capacity (FVC) below 0.70 or the lower limit of normal for age.
In Australia, the main guidelines used are the Australian Asthma Handbook and COPD-X Plan, which reflect GINA and GOLD recommendations.18,19
Coexisting asthma and COPD
GINA and GOLD developed documents that outlined best practice recommendations for asthma and COPD. This created the impression that the disorders were distinct and that treatment recommendations were quite different.
In 2015, both GINA and GOLD acknowledged that asthma and COPD coexist, not uncommonly, in the same individual, and termed this overlap ‘asthma–COPD overlap syndrome (ACOS)’. This was accompanied by a new, jointly produced statement on diagnosis and initial treatment of ACOS.20
Since then there has been considerable debate on whether this coexistence of two very common disorders should in fact be called a syndrome, and modifications may emerge as clarity improves. Nevertheless, there are sufficient concerns for patients who appear to have both conditions to warrant special considerations about diagnosis and management.
What do we know about ACOS?
The prevalence of ACOS has varied from 14 to 24% in patients with COPD, but this is highly dependent on the definition used.21-23 In a systematic review of 11 studies, definitions of ACOS varied from arguably the simplest, self-reported diagnosis of both asthma and COPD to those with more stringent objective criteria (e.g. spirometric demonstration of both obstruction and reversibility).23
Clinical implications of ACOS
In the systematic review of 11 studies, the researchers found that compared with patients with COPD alone, patients with ACOS had more symptoms of wheeze and cough, and a lower FEV1 and FEV1/FVC ratio despite having smoked fewer pack years.23 Patients with ACOS also experienced more frequent and more severe exacerbations..23 In contrast, another systematic review of 19 studies found no clinical differences between those with ACOS and COPD; this suggests there is a need to more carefully define ACOS.24
COPDGene study
The COPDGene study is an ongoing, cross-sectional survey of exsmoker, non-Hispanic white and African-American ex-smokers aged 45 to 80 years.25,26 Researchers are performing a genome-wide association study on the participants and correlating this with other respiratory data from history, spirometry and high-resolution chest CT.
COPDGene has reported on ACOS, defined by a formal diagnosis of asthma before age 40 years and a postbronchodilator FEV1/FVC ratio less than 0.70.25 Patients with ACOS were more likely to be female and African American. They had more severe and frequent exacerbations than patients with only COPD, and CT imaging showed less emphysema but more prominent bronchial wall thickening.25 The researchers identified three single nucleotide polymorphisms (in the genes CSMD1, SOX5 and GPR65) associated with ACOS, which may support defining a separate syndrome.25
ACOS in a COPD study cohort
In a Spanish cohort of 831 subjects with COPD, a diagnosis of ACOS was stringently defined by demonstration of one major criterion and two minor criteria.27 Major criteria included a history of asthma before age 40 years, a bronchodilator response greater than 400 mL or a 15% change in FEV1 ; minor criteria included bronchodilator response greater than 200 mL or a 12% change in FEV1 on two occasions, blood eosinophils greater than 5% or serum IgE above 100 IU/mL.27
The researchers found that ACOS had a prevalence of 15% in patients with COPD and the criteria were reproducible in 98% of patients one year later.27 They reported no differences between ACOS and COPD in regard to disease severity or comorbidities in this cohort, suggesting a more cautious approach to the use of a new syndrome in the diagnostic panorama.27
The same researchers compared two definitions of ACOS in a larger cohort of 3125 patients with COPD.23 Using a previous asthma diagnosis to define ACOS led to a prevalence of 15.9%, whereas using the more stringent definition above the prevalence was 5.1%.23Overall both definitions seemed to describe a population with similar characteristics that was more likely to be female and to have a greater bronchodilator reversibility, higher blood eosinophil counts and higher IgE levels.23
Difficulties diagnosing ACOS
Should we identify ACOS as a new separate syndrome? And if so, why should we do this? It might be simply a useful prognostic indicator within populations who have asthma or COPD, or it might have direct relevance for best management. The GINA–GOLD recommendations pose fresh approaches to treatment, although essentially considering treating the two diseases coexisting in one patient may prove to be satisfactory. So, if we do wish to distinguish a third disorder, ACOS, how should we diagnose it in clinical practice?
In both asthma and COPD, the need to perform spirometry is important for the correct diagnosis and when not performed leads to serious under- and overdiagnosis and a poor ability to differentiate between the two disorders.28,29 This situation is especially the case in patients who have features of both asthma and COPD, where confusion is likely to be compounded, and where without accurate diagnosis under- and overtreatment is more likely.
Bronchodilator reversibility
Bronchodilator reversibility or demonstration of reversible airflow obstruction is central in defining the presence of asthma. However, when it comes to patients with established fixed airflow obstruction – which is the central tenet for diagnosing COPD – it can be confusing.
A degree of reversible airflow obstruction, in the order of a change in FEV1 by at least 200 mL, or 12% from baseline, with a short-acting bronchodilator, occurs frequently in individuals with COPD. This reversibility is both highly variable and not reproducible, and alone it does not predict clinical course in COPD or asthma.30,31 Greater bronchodilator reversibility, such as 15% or at least 400 mL of FEV1, has been chosen as a major criterion to define ACOS because it is more likely to be reproducible and reflect variable airflow obstruction, but this has not been validated.27,32
Airway hyper-reactivity
Another important pathological feature of asthma is airway hyper-reactivity. Recently researchers examined the presence of airway hyper-reactivity to methacholine in two large cohorts – the Lung Health study (5887 patients with mild to moderate COPD) and the GLUCOLD study (51 patients with moderate to severe COPD).33
Airway hyper-reactivity was seen in 24% of COPD patients in the Lung Health Study and was associated with more rapid loss of lung function (FEV1 decline of 13.2 mL/year vs 12.4 mL/year) and a twofold increase in mortality.33 Although both findings are important surrogate outcomes in COPD, methacholine challenge testing is not practical for routine care in COPD.
Defining ACOS
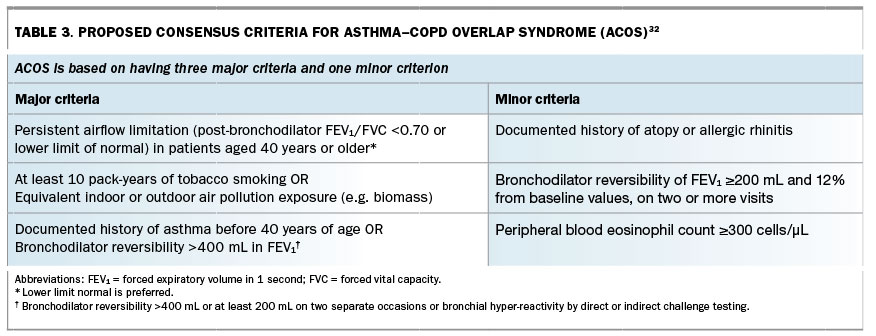
There are two main views regarding what is termed ACOS. In one, the coexistence of asthma and COPD is acknowledged to occur but it is not considered to be a syndrome. In the other, ACOS is strongly supported, and a recent ‘roundtable’ consensus document was published to attempt a clearer definition of ACOS, at least for the purposes of future assessments and clinical trials.32 This definition was based on meeting three major criteria and one minor criterion (Table 3).32
{kind=link}
Targeting treatment
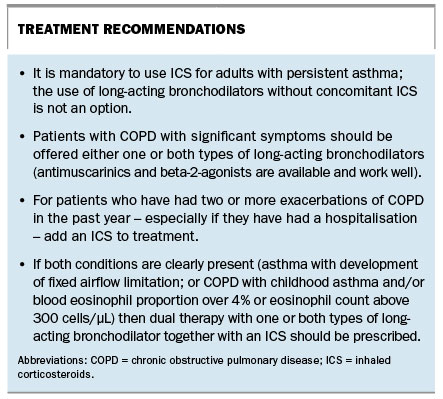
ICS are recommended treatment for all adult patients with persistent asthma, but in COPD their use is reserved for those with a previous history of exacerbations and more severe disease, to prevent exacerbations.18 However, ICS use in COPD has been associated with an increased risk of pneumonia, as well as other adverse effects seen in older populations.34 In ACOS, guidelines recommend the combined use of ICS and long-acting bronchodilators as first-line therapy.16,35
Eosinophilia as a biomarker
Recently a biomarker has emerged that may predict response to ICS in COPD – the presence of eosinophilic airway inflammation, a characteristic that in the past seemed to be more consistent with asthma than with COPD.
Sputum eosinophilia in COPD has been found to predict short-term clinical responses to ICS.36 It is not easy or routine even in specialist settings to measure sputum inflammatory cells, and more recently it has been shown that blood eosinophils can be used to predict the presence of airway eosinophilia.37 In two large interventional trials in patients with COPD, those with higher blood eosinophil counts were found to respond best to ICS and this was associated with reduced exacerbation risk.38,39 These observations, it must be said, are at present from uncontrolled, retrospective analyses, and prospective evaluation is desperately needed.
Researchers are now so interested in blood eosinophils as a treatable biomarker that trials are underway to use anti-IL5 monoclonal antibody therapy (mepolizumab and benralizumab) to prevent exacerbations in COPD, stratifying subjects by blood eosinophil count. Furthermore, there is growing evidence that pneumonia risk associated with the use of ICS in COPD may be predicted by lower eosinophil counts (below 2%). If proven in prospective research, this finding may add further impetus to incorporating blood eosinophilia in guideline-based therapy for COPD as well as asthma.40
How do we treat patients with asthma, COPD or ACOS?
In the future we hope that the diagnostic criteria and phenotyping for both asthma and COPD – and perhaps ACOS – will be clarified by the extensive research currently underway. Until then, we can provide the treatment advice in the Box.
{kind=link}
Conclusion
In the 1950s and 1960s, our predecessors experienced a greater understanding of the pathology and physiology of airways disease and, accordingly, they adapted their thinking and management strategies. We now face a similar increase in our knowledge of the molecular and genetics pathways that underlie the development of asthma and COPD.
This process is still in evolution and like any change will lead to some uncertainty and even confusion. Nonetheless, a greater understanding of the processes underlying airway diseases and more precise targeting of treatments will inevitably lead to better patient outcomes – more efficacious interventions with fewer adverse events. Is ACOS a distinct syndrome, separate from asthma and COPD? We cannot be adamant one way or the other; however, there are useful and relatively simple guiding principles for practice as outlined in this review.
COMPETING INTERESTS: Professor Wark has participated on advisory boards for Vertex and Novartis. He has spoken at meetings sponsored by AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Vertex and Novartis. Professor Frith has received honoraria and third-party travel for educational, advisory board work in the past five years from AstraZeneca, GlaxoSmithKline, CSL, Novartis, Boehringer Ingelheim, Menarini and Mundipharma; and is a member of the Boards of Directors for Lung Foundation Australia and Global Initiative for COPD (GOLD) and of the COPD Co-ordinating Committee and Executive for Lung Foundation Australia, for which third-party travel arrangements have been accepted.