Community-acquired pneumonia in adults: current challenges and recommendations

Lung diseases
Evidence is growing that clinical diagnosis of community-acquired pneumonia (CAP) is inaccurate. Viruses are increasingly recognised in patients with CAP, although their significance is often unclear. Prompt initial management is important for patients with CAP, and best outcomes are achieved with a ‘CAP bundle of care’ approach involving early treatment with guideline-concordant antibiotics and early mobilisation. Reducing cardiovascular risk after pneumonia is an emerging challenge.
- Community-acquired pneumonia (CAP) is prevalent, and causative pathogens are evolving over time.
- The combination of a beta-lactam with a macrolide antibiotic remains the optimal therapy in patients hospitalised with CAP in Australia.
- Beta-lactam monotherapy, typically amoxicillin, is sufficient for most patients with CAP who are judged suitable for treatment in the community in Australia.
- Cardiovascular events are common in patients with pneumonia both during the acute illness and in the following six to 12 months, with significant implications for general practice follow up of these patients.
- There is increasing focus on a ‘CAP bundle of care’ approach to ensure each patient receives optimal care.
- The benefit of corticosteroid therapy in patients with CAP is a subject of debate; it is currently recommended in patients with critically severe disease (i.e. requiring intensive care).
Picture credit: © Kevin Somerville/Medical Images
Pneumonia is a major health concern worldwide in both hospital and community settings, causing significant morbidity and mortality. When pneumonia occurs in patients without recent (in the previous 30 days) or current hospitalisation and without known immunocompromise, it is termed community-acquired pneumonia (CAP). The reliability of a clinical diagnosis of CAP has been challenged recently. The contribution of viruses to CAP is increasingly recognised. There is now a growing focus on ‘CAP bundle of care’ treatment and recognition of the importance of treating comorbidities and considering cardiovascular risk after CAP. This article discusses current challenges and recommendations in diagnosis and management of patients with CAP.
Burden of community-acquired pneumonia
In Australia, pneumonia leads to 200 hospital admissions for every 100,000 adults each year, accounting for 2% of all hospitalisations.1 Although patients with CAP are usually managed in the community, most pneumonia-related mortality, healthcare burden and cost occurs among patients who are hospitalised with CAP.2 Between July 2011 and June 2012, there were 129,393 hospitalisations in Australia with respiratory infection as the principal diagnosis, mostly due to pneumonia.3 The direct healthcare costs of pneumonia in Australia are therefore considerable, but the indirect costs, including long-term complications, are likely to be substantially higher.
Challenges in diagnosis of CAP
CAP is usually diagnosed based on the presence of the following three criteria:
- symptoms (cough, rigors, dyspnoea and chest pain)
- clinical signs (fever, crackles and bronchial breathing)
- a chest x-ray showing an infiltrate consistent with pulmonary consolidation.
Although this seems straightforward, establishing the diagnosis of CAP radiologically in patients with underlying respiratory disease such as pulmonary fibrosis, bronchiectasis or lung cancer can be problematic. Indeed, substantial evidence suggests that even radiologists often disagree on the presence or absence of pneumonia on plain chest x-rays.4,5
Recent studies have challenged the accuracy of a clinical diagnosis of pneumonia. A Belgian group prospectively studied the potential role of CT scanning in 319 patients with suspected pneumonia.6 Clinicians treating patients presenting to hospital with symptoms consistent with CAP were asked to diagnose pneumonia based on clinical assessment (history and examination) plus the chest x-ray appearance. Patients then underwent CT to assess for evidence of pneumonia, and results were compared with the clinical diagnosis. Discordance between the clinical diagnosis and CT results was found in nearly 40% of patients. Importantly, nearly one-third of patients diagnosed with pneumonia by clinicians had no pulmonary infiltrate on CT. This finding may explain discrepancies between the results of previous studies of CAP.7
In a smaller study of 77 outpatients with CAP, chest x-ray findings were compared with CT MRI findings at the time of diagnosis and 30 days later.8 Pneumonia was identified in 32 patients by CT scan, 30 by MRI and 23 by chest x-ray. The false-positive rate was much lower in this study, with only four false positives on chest x-ray (and none on MRI), but all imaging was interpreted by a radiologist rather than by the treating clinician, and the 30-day follow-up studies were available for comparison.
In most settings it is currently impractical, and probably not in patients’ best interests, to perform a CT chest scan as part of routine clinical care in patients with suspected pneumonia. More data are needed before we can fully understand the meaning of a disparity between clinical assessment and CT scan findings in terms of pathogens, patient outcomes and treatment selection. It is, however, important that clinicians are aware of the limitations of chest x-rays and do not either discount pneumonia, particularly if the patient has evidence of cardiac or respiratory compromise, or overdiagnose pneumonia and forget about alternative diagnoses that may require different treatment.
Pathogens causing CAP in Australia
Almost all aetiological studies of CAP have identified Streptococcus pneumoniae as the most common pathogen. Although there is some evidence suggesting that the incidence of disease caused by S. pneumoniae is decreasing because of the newer conjugate pneumococcal vaccines, S. pneumoniae remains the most commonly identified cause of pneumonia. Other bacteria that cause CAP vary by location and population. They include Haemophilus influenzae, Mycoplasma pneumoniae, group A streptococci, Legionella spp., Chlamydophila pneumoniae and Moraxella catarrhalis.9
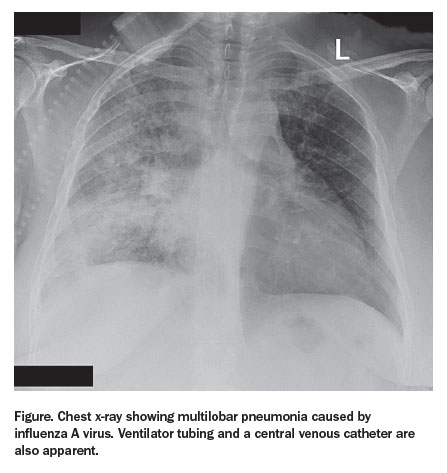
Viruses such as influenza A and B viruses, respiratory syncytial virus, adenovirus and a variety of coronaviruses have also been recognised as causes of CAP, either as the sole organism or as a coexisting pathogen (Figure). Improved diagnostic techniques such as nucleic acid amplification assays have increased the frequency with which multiple pathogens are detected, especially a virus and a bacterium, now approaching 25% in recent studies.10,11 A key unresolved issue is whether the detection of a virus in upper airways secretions represents the cause of pneumonia, particularly when multiple pathogens are detected, or a resolving prior infection that predisposed to bacterial pneumonia.
{kind=link}
Although there has been no detailed aetiological study of CAP in Australia for more than a decade, earlier studies found similar pathogens to international published series.12,13 A key exception is in patients with CAP in tropical Australia, where other organisms should be considered, including Burkholderia pseudomallei, the cause of melioidosis, and Acinetobacter spp. Both of these organisms are prevalent, particularly in severe cases of CAP, and neither is covered by standard empirical CAP therapy. 14,15
Current management recommendations for CAP
Treatment in the community
The decision whether to admit a patient with CAP to hospital depends on factors such as illness severity, age, comorbidities, functional status and living arrangement. Risk assessment tools such as the Pneumonia Severity Index (PSI) and CURB-65 (Confusion, blood Urea nitrogen, Respiratory rate, Blood pressure, age 65 years or older) can help determine whether patients may be safely treated in the community.16-19 Clinical assessment, however, remains paramount, particularly in younger patients, in whom these scoring systems may underestimate the severity of illness.
Despite recent advances in rapid diagnosis, the causative pathogen of CAP is almost never known at the time of initiating treatment. For treatment in the community, there is no evidence to support any specific pathogen testing at the time of initial therapy. Therefore empirical antibiotic therapy remains the standard of care for patients diagnosed with CAP and should be commenced as soon as the diagnosis is made.9
For patients with CAP assessed as appropriate for treatment in the community in Australia, a beta-lactam such as amoxicillin at a dose of 1 g three times a day for a normal adult is probably sufficient for those without chronic lung disease.20 In those with chronic lung disease, it is recommended to consider a combination of a beta-lactam and a beta-lactamase inhibitor (such as amoxicillin–clavulinic acid) because of the risk of the presence of beta-lactamase producing organisms (e.g. Haemophilus influenzae) selected by prior antibiotic use.21 The evidence supporting a need to cover Mycoplasma, Chlamydia and Legionella species in outpatients is poor, and this cover should probably be reserved for patients who do not respond to initial beta-lactam therapy.22 In patients with mild penicillin allergy, a second-generation cephalosporin such as cefuroxime or cefalexin may be appropriate. In those with significant penicillin allergy, alternatives include doxycycline, a macrolide such as roxithromycin or clarithromycin, or trimethoprim–sulfamethoxazole.
A recent report based on pooled culture data from multiple settings found that the rate of penicillin resistance among isolates from patients with CAP in the community in Australia was 1.3%.23 Most resistance is not of a level likely to cause clinical failure. In organisms obtained from noninvasive samples (not blood cultures), resistance rates were greater than 25% for erythromycin and tetracycline and just below 30% for trimethoprim–sulfamethoxazole, supporting the preference for beta-lactam or cephalosporin-based therapy. Moxifloxacin is another alternative but should probably be reserved for hospitalised patients.
Given the high incidence of viral pathogens in patients with pneumonia, the question arises whether to administer anti-influenza treatment to patients with pneumonia when influenza is circulating in the community. Meta-analysis of a considerably conflicted evidence base suggests that oseltamivir treatment of patients with CAP in the community may have a small beneficial effect on subsequent pneumonia and hospitalisation rates.24 On the other hand, concern persists about use of oseltamivir in outpatients, predominantly that excess use in this setting will drive up resistance rates. However, in the absence of cheap, reliable point-of-care tests for influenza, the benefits of oseltamivir probably outweigh the risks in patients who clearly have pneumonia and symptoms consistent with an influenza illness when influenza is known to be circulating in the community.
Inpatient treatment
In patients admitted to hospital there is a philosophical argument in favour of identifying the pathogen, but no data to suggest that this improves patient outcomes.25 Although new diagnostic platforms are emerging that promise rapid, accurate pathogen identification, treatment remains empirical.
Dual-antibiotic therapy has become the standard of care for patients with CAP requiring inpatient treatment since a series of retrospective studies in the early 2000s suggested that a combination of antibiotics, particularly a beta-lactam and a macrolide, was associated with significantly better outcomes, particularly in patients with severe bacteraemic pneumococcal disease.25 Recent analyses suggest that the addition of a macrolide to a beta-lactam has reduced mortality from severe CAP by at least a third.26
However, debate over combination therapy continues and was not resolved by two recent prospective trials. A Swiss study did not find that beta-lactam monotherapy was as safe as beta-lactam plus macrolide combination therapy.27 In contrast, a Dutch trial reported no significant difference in outcomes between beta-lactam monotherapy and combination therapy.28 However, this trial had major problems, including no radiological evidence of pneumonia in 25% of patients, administration of a macrolide to 43% of supposed monotherapy patients, and major differences in choice of beta-lactam and macrolide between the two groups.
Consequently, combination therapy with a beta-lactam and a macrolide remains the standard of care for patients hospitalised with pneumonia. In most patients, the combination of amoxicillin and a macrolide is probably sufficient, but in those who are critically ill a third-generation cephalosporin such as ceftriaxone or cefotaxime is preferred to amoxicillin because of the high mortality associated with inadequate empirical therapy in this group.25
Some Australian guidelines recommend a tetracycline, and especially doxycycline, as the ‘atypical’ coverage component of dual antibiotic therapy.20 Although it is possible that a tetracycline confers the same benefit as a macrolide, there are few data supporting tetracyclines compared with a large number of studies in favour of macrolides. In part, the controversy persists because the mechanism for the survival advantage with macrolide therapy is unclear. However, it is almost certainly not due to coverage of pathogens such as Legionella and Mycoplasma spp. but due to a mix of anti-inflammatory and antitoxin effects.25
Given the high mortality of patients admitted to intensive care units with pneumonia (typically 25% or greater), a search for alternative therapies continues. Recent meta-analyses have sparked a significant debate over the benefit of corticosteroids in patients with CAP.29-31 Despite many large randomised controlled studies showing unimpressive results, pooled analyses suggest reduced mortality in high-risk patients. The meta-analyses, however, are flawed as the only two studies showing a survival advantage had significant methodological problems.32,33 There are also concerns about increased mortality in patients with influenza pneumonia who are treated with corticosteroids.34,35 At present, corticosteroid therapy cannot be recommended in patients with CAP and certainly not in those in whom influenza has been excluded. We need a much better understanding of which patients might benefit from corticosteroids.
Increasing evidence of acute cardiovascular events associated with pneumonia
Increased cumulative rates of cardiac failure (14%), arrhythmia (5%) and myocardial infarction (5%) have all been seen in patients with CAP during hospitalisation.36 Clinical studies have documented two- to eightfold increases in the risk of cardiovascular disease within the first 30 days after respiratory infections.37
Several studies have assessed whether aspirin can reduce acute cardiovascular events in patients with pneumonia. Only one small randomised study has been published, and it showed a substantial reduction in myocardial infarction associated with daily therapy with 300 mg of aspirin for one month.38 Several retrospective studies also suggest a lower cardiovascular risk in patients taking aspirin, clopidogrel or ticagrelor.39-42
Although we need more data to make an absolute recommendation on use of daily aspirin in patients with CAP, the failure of a dose of 100 mg to reduce cardiovascular events or platelet activation suggests a higher dose of 300 mg will likely be required.43 For the moment, clinicians should remember the key point that acute cardiac complications are common in patients with CAP and should consider whether the risk can be reduced, especially in patients with known cardiovascular risk factors.
Shifting focus from acute to longer-term outcomes of CAP
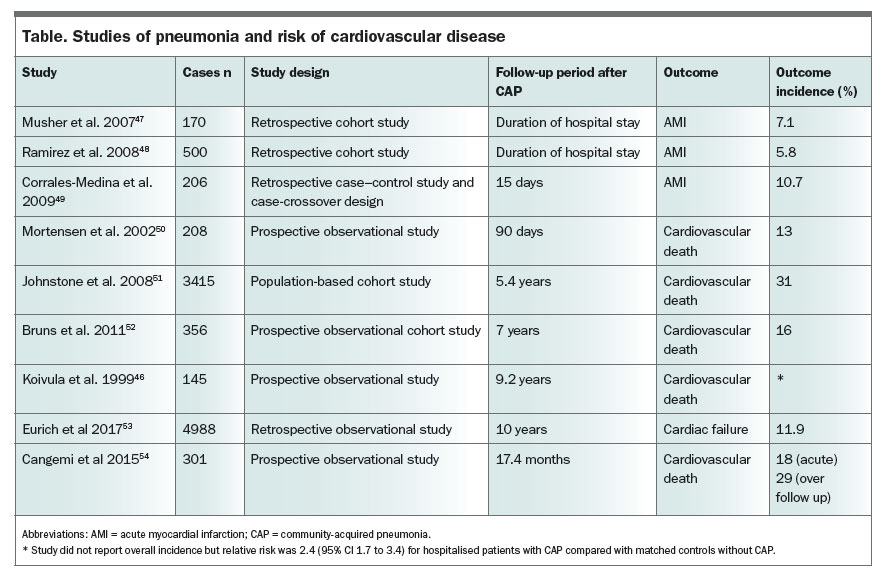
It is now clear that the risk of death associated with pneumonia does not cease with resolution of the acute infection, especially in elderly patients with comorbid disease. The primary cause of later mortality appears to be an increase in cardiovascular events over a two to five-year period.37,44-46 Studies showing the reported associations between pneumonia and cardiac disease are summarised in the Table.46-54
{kind=link}
In the first 90 days after discharge from hospital, mortality is highest in patients with the highest markers of inflammation.55 Predicting subsequent risk over the next two to five years is not as clear and requires research. Notably, this added mortality is seen even in patients who were apparently healthy before admission with pneumonia.44
Although we do not currently know how to reduce mortality and morbidity in CAP survivors, it seems logical that measures to reduce acute cardiac injury at the time of pneumonia should have some impact. Whether longer-term anti-inflammatory or antiplatelet therapy is of value remains to be tested, but the realisation that pneumonia has significant long-term consequences that far outweigh the acute burden is a major paradigm shift for physicians treating patients with CAP.
CAP bundle of care treatment
Bundles of care are more than just a group of interventions; they are a process designed so that each patient receives the optimal care every time, based on the best available evidence. A pilot program in the UK showed a reduction in 30-day inpatient mortality from CAP, from 13.6% to 8.8%, with the use of a CAP care bundle focused on using guideline-based empirical therapy and early administration of antibiotics.56
Extrapolation from the available data suggests that the following interventions are likely to be included in future CAP bundles of care:
- use of a validated CAP severity score to aid in clinical evaluation and deciding the site of care (in the community or hospital)
- prompt administration of empirical antibiotics including a beta-lactam and a macrolide (ideally within three hours of presentation)
- rapid attention to metabolic issues such as adequate fluid resuscitation and correcting electrolyte disturbances and hyperglycaemia
- early identification and treatment of type II respiratory failure (hypoxaemia with hypercapnia)
- appropriate thromboembolic prophylaxis
- encouraging early ambulation
- addressing cardiovascular risk factors, and possibly prescribing antiplatelet therapy.
Conclusion
CAP is prevalent both in Australia and worldwide and is an important cause of mortality and morbidity. Causative pathogens are evolving over time, with pneumococcal conjugate vaccine being a major driver of the change. New diagnostic tests are also changing our perspective on the proportion of patients with multiple pathogens and the high frequency of viral pneumonia.
There is now increasing focus on CAP bundle of care treatment, with recognition of the importance of treating comorbidities, thromboembolic prophylaxis, aspirin treatment and early mobilisation. The relative contribution of each component of a future bundle remains to be clearly determined. Prompt antibiotic treatment is important, and the combination of a beta-lactam and a macrolide remains the optimal therapy in patients hospitalised for CAP, whereas beta-lactam monotherapy is probably adequate for those who are considered suitable for treatment in the community.
The benefit of corticosteroid therapy in patients hospitalised for CAP is unclear, and further elucidation of the risks and benefits to individuals is needed. Cardiovascular events are common in patients with pneumonia, and this risk needs to be addressed. With the increasing recognition of the long-term health outcomes of CAP survivors, clinicians require a major shift in thinking to include long-term preventive management. Further studies are desperately needed to determine which patients are at highest risk and how that risk can be ameliorated. RMT
References
- Tsirgiotis E, Ruffin R. Community acquired pneumonia. A perspective for general practice. Aust Fam Physician 2000; 29: 639-645.
- Ramirez JA, Anzueto AR. Changing needs of community-acquired pneumonia. J Antimicrob Chemother 2011; 66 Suppl 3: iii3-iii9.
- Poulos L, Correll P, Toelle B, Reddel H, Marks G. Lung disease in Australia. Brisbane: Lung Foundation Australia; 2014.
- Hopstaken RM, Witbraad T, van Engelshoven JM, Dinant GJ. Inter-observer variation in the interpretation of chest radiographs for pneumonia in community-acquired lower respiratory tract infections. Clin Radiol 2004; 59: 743-752.
- Albaum MN, Hill LC, Murphy M, et al. Interobserver reliability of the chest radiograph in community-acquired pneumonia. PORT Investigators. Chest 1996; 110: 343-350.
- Claessens YE, Debray MP, Tubach F, et al. Early chest computed tomography scan to assist diagnosis and guide treatment decision for suspected community-acquired pneumonia. Am J Respir Crit Care Med 2015; 192: 974-982.
- Waterer GW. The diagnosis of community-acquired pneumonia. Do we need to take a big step backward? Am J Respir Crit Care Med 2015; 192: 912-913.
- Syrjala H, Broas M, Ohtonen P, Jartti A, Paakko E. Chest magnetic resonance imaging for pneumonia diagnosis in outpatients with lower respiratory tract infection. Eur Respir J 2017; 49: pii: 1601303.
- Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007; 44 Suppl 2: S27-S72.
- Holter JC, Muller F, Bjorang O, et al. Etiology of community-acquired pneumonia and diagnostic yields of microbiological methods: a 3-year prospective study in Norway. BMC Infect Dis 2015; 15: 64.
- Jain S, Self WH, Wunderink RG, et al. Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med 2015; 373: 415-427.
- Charles PG, Whitby M, Fuller AJ, et al. The etiology of community-acquired pneumonia in Australia: why penicillin plus doxycycline or a macrolide is the most appropriate therapy. Clin Infect Dis 2008; 46: 1513-1521.
- Wilson PA, Ferguson J. Severe community-acquired pneumonia: an Australian perspective. Intern Med J 2005; 35: 699-705.
- Stephens DP, Thomas JH, Ward LM, Currie BJ. Melioidosis causing critical illness: a review of 24 years of experience from the Royal Darwin Hospital ICU. Crit Care Med 2016; 44: 1500-1505.
- Davis JS, McMillan M, Swaminathan A, et al. A 16-year prospective study of community-onset bacteremic Acinetobacter pneumonia: low mortality with appropriate initial empirical antibiotic protocols. Chest 2014; 146: 1038-1045.
- Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med 1997; 336: 243-250.
- Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax 2003; 58: 377-382.
- Fine MJ, Hough LJ, Medsger AR, et al. The hospital admission decision for patients with community-acquired pneumonia. Results from the pneumonia Patient Outcomes Research Team cohort study. Arch Intern Med 1997; 157: 36-44.
- Capelastegui A, Espana PP, Quintana JM, et al. Validation of a predictive rule for the management of community-acquired pneumonia. Eur Respir J 2006; 27: 151-157.
- Therapeutic Guidelines Expert Groups. eTG complete. Melbourne: Therapeutic Guidelines Ltd. Available online at: http://www.tg.org.au (accessed April 2017).
- Van Eldere J, Slack MP, Ladhani S, Cripps AW. Non-typeable Haemophilus influenzae, an under-recognised pathogen. Lancet Infect Dis 2014; 14: 1281-1292.
- Lim WS, Baudouin SV, George RC, et al. BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax 2009; 64 Suppl 3: iii1-iii55.
- Australian Commission on Safety and Quality in Health Care (ACSQHC). AURA 2016: first Australian report on antimicrobial use and resistance in human health. Sydney: ACSQHC; 2016.
- Lipsitch M, Hernan MA. Oseltamivir effect on antibiotic-treated lower respiratory tract complications in virologically positive randomized trial participants. Clin Infect Dis 2013; 57: 1368-1369.
- Wunderink RG, Waterer GW. Community-acquired pneumonia. N Engl J Med 2014; 370: 1863.
- Gattarello S, Borgatta B, Sole-Violan J, et al. Decrease in mortality in severe community-acquired pneumococcal pneumonia: impact of improving antibiotic strategies (2000-2013). Chest 2014; 146: 22-31.
- Garin N, Genne D, Carballo S, et al. ββ-Lactam monotherapy vs ββ-lactam-macrolide combination treatment in moderately severe community-acquired pneumonia: a randomized noninferiority trial. JAMA Intern Med 2014; 174: 1894-1901.
- Postma DF, van Werkhoven CH, van Elden LJ, et al. Antibiotic treatment strategies for community-acquired pneumonia in adults. N Engl J Med 2015; 372: 1312-1323.
- Siemieniuk RA, Meade MO, Alonso-Coello P, et al. Corticosteroid therapy for patients hospitalized with community-acquired pneumonia: a systematic review and meta-analysis. Ann Intern Med 2015; 163: 519-528.
- Horita N, Otsuka T, Haranaga S, et al. Adjunctive systemic corticosteroids for hospitalized community-acquired pneumonia: systematic review and meta-analysis 2015 update. Sci Rep 2015; 5: 14061.
- Chen LP, Chen JH, Chen Y, Wu C, Yang XH. Efficacy and safety of glucocorticoids in the treatment of community-acquired pneumonia: a meta-analysis of randomized controlled trials. World J Emerg Med 2015; 6: 172-178.
- Nafae R, Ragab M, Amany F, Rashed S. Adjuvant role of corticosteroids in the treatment of community-acquired pneumonia. Egypt J Chest Dis Tuberculosis 2013; 62: 439-445.
- Confalonieri M, Urbino R, Potena A, et al. Hydrocortisone infusion for severe community-acquired pneumonia: a preliminary randomized study. Am J Respir Crit Care Med 2005; 171: 242-248.
- Yang JW, Fan LC, Miao XY, et al. Corticosteroids for the treatment of human infection with influenza virus: a systematic review and meta-analysis. Clin Microbiol Infect 2015; 21: 956-963.
- Cao B, Gao H, Zhou B, et al. Adjuvant corticosteroid treatment in adults with influenza a (H7N9) viral pneumonia. Crit Care Med 2016; 44: e318-e328.
- Corrales-Medina VF, Taljaard M, Yende S, et al. Intermediate and long-term risk of new-onset heart failure after hospitalization for pneumonia in elderly adults. Am Heart J 2015; 170: 306-312.
- Corrales-Medina VF, Alvarez KN, Weissfeld LA, et al. Association between hospitalization for pneumonia and subsequent risk of cardiovascular disease. JAMA 2015; 313: 264-274.
- Oz F, Gul S, Kaya MG, et al. Does aspirin use prevent acute coronary syndrome in patients with pneumonia: multicenter prospective randomized trial. Coron Artery Dis 2013; 24: 231-237.
- Falcone M, Russo A, Cangemi R, et al. Lower mortality rate in elderly patients with community-onset pneumonia on treatment with aspirin. J Am Heart Assoc 2015; 4: e001595.
- Falcone M, Russo A, Farcomeni A, et al. Septic shock from community-onset pneumonia: is there a role for aspirin plus macrolides combination? Intensive Care Med 2016; 42: 301-302.
- Gross AK, Dunn SP, Feola DJ, et al. Clopidogrel treatment and the incidence and severity of community acquired pneumonia in a cohort study and meta-analysis of antiplatelet therapy in pneumonia and critical illness. J Thromb Thrombolysis 2013; 35: 147-154.
- Storey RF, James SK, Siegbahn A, et al. Lower mortality following pulmonary adverse events and sepsis with ticagrelor compared to clopidogrel in the PLATO study. Platelets 2014; 25: 517-525.
- Cangemi R, Casciaro M, Rossi E, et al. Platelet activation is associated with myocardial infarction in patients with pneumonia. J Am Coll Cardiol 2014; 64: 1917-1925.
- Waterer GW, Kessler LA, Wunderink RG. Medium-term survival after hospitalization with community-acquired pneumonia. Am J Respir Crit Care Med 2004; 169: 910-914.
- Mortensen EM, Kapoor WN, Chang CC, Fine MJ. Assessment of mortality after long-term follow-up of patients with community-acquired pneumonia. Clin Infect Dis 2003; 37: 1617-1624.
- Koivula I, Sten M, Makela PH. Prognosis after community-acquired pneumonia in the elderly: a population-based 12-year follow-up study. Arch Intern Med 1999; 159: 1550-1555.
- Musher DM, Rueda AM, Kaka AS, Mapara SM. The association between pneumococcal pneumonia and acute cardiac events. Clin Infect Dis 2007; 45: 158-165.
- Ramirez J, Aliberti S, Mirsaeidi M, et al. Acute myocardial infarction in hospitalized patients with community-acquired pneumonia. Clin Infect Dis 2008; 47: 182-187.
- Corrales-Medina VF, Serpa J, Rueda AM, et al. Acute bacterial pneumonia is associated with the occurrence of acute coronary syndromes. Medicine (Baltimore) 2009; 88: 154-159.
- Mortensen EM, Coley CM, Singer DE, et al. Causes of death for patients with community-acquired pneumonia: results from the Pneumonia Patient Outcomes Research Team cohort study. Arch Intern Med 2002; 162: 1059-1064.
- Johnstone J, Eurich DT, Majumdar SR, Jin Y, Marrie TJ. Long-term morbidity and mortality after hospitalization with community-acquired pneumonia: a population-based cohort study. Medicine (Baltimore) 2008; 87: 329-334.
- Bruns AH, Oosterheert JJ, Cucciolillo MC, et al. Cause-specific long-term mortality rates in patients recovered from community-acquired pneumonia as compared with the general Dutch population. Clin Microbiol Infect 2011; 17: 763-768.
- Eurich DT, Marrie TJ, Minhas-Sandhu JK, Majumdar SR. Risk of heart failure after community acquired pneumonia: prospective controlled study with 10 years of follow-up. BMJ 2017; 356: j413.
- Cangemi R, Calvieri C, Falcone M, et al; SIXTUS Study Group. Relation of cardiac complications in the early phase of community-acquired pneumonia to long-term mortality and cardiovascular events. Am J Cardiol 2015; 116: 647-651.
- Yende S, D’Angelo G, Kellum JA, et al. Inflammatory markers at hospital discharge predict subsequent mortality after pneumonia and sepsis. Am J Respir Crit Care Med 2008; 177: 1242-1247.
- Lim WS, Rodrigo C, Turner AM, Welham S, Calvert JM, British Thoracic S. British Thoracic Society community-acquired pneumonia care bundle: results of a national implementation project. Thorax 2016; 71: 288-290.