Haemangiomas. Treating those that won’t fade away

Infant and newborn care
Haemangiomas are the most common tumours of infancy. Haemangiomas that may be life-threatening or cause physical deformity should be referred early for assessment and management. Treatment can also be considered for anticipated cosmetic impact. This article discusses how to diagnose infantile haemangiomas, differential diagnoses to consider, when to refer and treatment options.
- Infantile haemangiomas are benign tumours.
- They are the most common tumours of infancy.
- Most haemangiomas involute and do not require treatment.
- Haemangiomas requiring treatment should be identified.
- Oral propranolol is the preferred treatment for infantile haemangiomas.
Infantile haemangiomas are benign tumours that comprise proliferating vascular endothelial cells. The most common tumours of infancy, haemangiomas occur in up to 4% of babies and are more common in female and premature babies. Most haemangiomas do not require treatment due to their natural history of spontaneous involution. However, some haemangiomas cause complications such as ulceration and cosmetic disfigurement. In addition, they may compromise vision, hearing or breathing. This article guides decision-making around how to manage haemangiomas, including identifying haemangiomas that need therapy and recommended therapies.
Natural history of haemangiomas
Haemangiomas usually present in the first weeks of life. They start as a red or bruise-like stain in the skin. The area involved is generally mapped out at the onset – the haemangioma will grow higher but will not spread laterally into surrounding areas. They usually stop growing by four months of age, but larger haemangiomas may grow until 18 months of age. When the growth period ceases, the colour of the haemangioma will move from a vibrant strawberry red to a darker purple-red colour. It will also become a little softer, and grey-white flecks will start to break up the colour. Thereafter haemangiomas slowly improve and most will disappear eventually without trace.
The rate of involution is variable and only 10% will have cleared by one year of age. Most haemangiomas will involute from 1 to 10 years of age, with larger haemangiomas generally taking longer to resolve. Not all haemangiomas resolve without trace; some leave permanent telangiectasia, scarring (particularly following ulceration), stretched and inelastic skin (like a circular striae), or excess fibro-fatty tissue (usually in those that had deep and superficial components).1
Establishing the diagnosis
Most haemangiomas are not difficult to diagnose, but other diagnoses need to be considered in some circumstances. Another diagnosis should be considered for any vascular mass present at birth, including other benign growths such as congenital haemangiomas – divided into rapidly involuting (Figure 1) and noninvoluting – venous, arterovenous and lymphatic malformations, and infantile myofibromas.2,3 More rarely, but importantly, sarcomas of various types have been misdiagnosed as haemangiomas.
{kind=link}
Haemangiomas may be present at birth but should not be fully formed. A growth phase after birth is an essential characteristic of haemangiomas. Consider an alternative diagnosis in any stain or plaque that does not evolve. Differentials can include a capillary malformation, angiokeratoma and glomuvenous malformation.2,3
Subclassification of infantile haemangiomas
Haemangiomas may be focal or segmental. Focal haemangiomas are usually circular or oval shaped and do not respect or align in any embryological or cosmetic boundaries. Segmental haemangiomas are larger, with their shape following embryological planes, and are cut off midline (Figure 2). Haemangiomas that cannot be easily categorised as focal or segmental are referred to as ‘indeterminate’.
{kind=link}
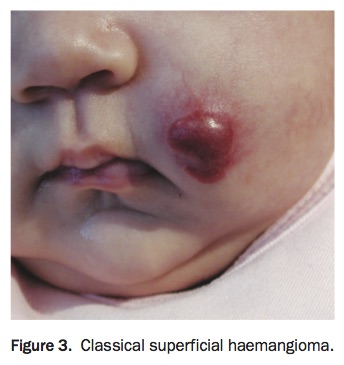
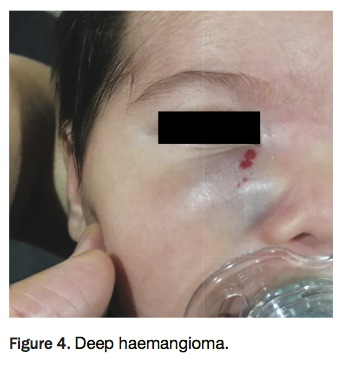
With regard to morphology, haemangiomas are described as superficial, deep or mixed. The superficial component is in the superficial part of the dermis and gives the classic ‘strawberry’ appearance (Figure 3). The deep component is subcutaneous and will present clinically as a soft, warm and bluish mass (Figure 4). Deep haemangiomas do not have the diagnostic strawberry colour, so clinical diagnosis may not be as definitive. Although ultrasound can aid with diagnosis, it can only determine that the mass is very vascular. For those that are mixed, the superficial and deep components do not necessarily grow and fade in unison. Often the superficial component of the haemangioma will have started involution while the deeper component continues to grow.
{kind=link}
{kind=link}
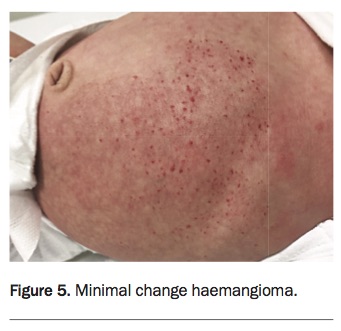
Rarely, haemangiomas will remain primarily as a stain in the skin, with very little or no elevation. These are referred to as ‘minimal change haemangiomas’ (Figure 5). The development of smaller red blebs can help to distinguish these from capillary malformations.
{kind=link}
Assessing a child with an infantile haemangioma
When assessing the child, it is essential to take a thorough medical history and clinical examination (including heart rate). Further investigations are only indicated based on abnormal findings from the history and/or clinical examination.4
Further investigation may be appropriate in the following situations:
- Beard distribution haemangiomas. These are frequently associated with airway haemangiomas. Refer for specialist assessment with laryngoscopy.
- Segmental head and neck infantile haemangiomas. These are associated with increased risk of PHACE syndrome (potential abnormalities of eyes, brain, heart and major arteries). Urgent referral to a specialist centre is required in this setting.
- Segmental lumbar and pelvic haemangiomas. These can be associated with anogenital, renal or spinal anomalies. Consider ultrasound or MRI spine, and renal ultrasound.
- Patients with more than five infantile haemangiomas. In this setting, there is a risk of associated internal haemangiomas including in the liver. Those in the liver can create an arteriovenous shunt and impact cardiac output. Clinical assessment, along with an ultrasound of the abdomen, is warranted.
- Very large infantile haemangiomas. These are associated with hypothyroidism and high output cardiac failure.
The following framework for treating haemangiomas was developed by members of the Australasian Vascular Anomalies Network and the Australasian Paediatric Dermatology Network and has been used with permission.5
Indications for treatment
- Life- or function-threatening infantile haemangiomas
- Airway haemangioma or potential for this (beard haemangioma)
- Potential for visual impairment; haemangiomas involving eyelids can lead to risk of amblyopia from eye occlusion, or pressure-induced astigmatism
- Spinal cord involvement
- High flow and cardiac compromise, e.g. large hepatic lesions
- Haemangiomas causing hypothyroidism
- Large haemangiomas interfering with physical development
- Systemic haemangiomatosis.
Ulcerated haemangiomas
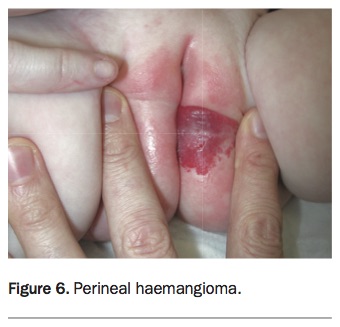
Ulceration of haemangiomas tends to occur in the early proliferative phase and is more common with larger haemangiomas and those in mobile areas of skin and skin folds. The ulceration tends to result in scarring and often causes significant pain. Sites such as the lip and perineum (Figure 6) are the most prone. Sizeable haemangiomas at these sites should be treated before ulceration develops.6 If there is inadequate response to standard wound care, consider laser treatment or early surgery as well as propranolol.
{kind=link}
Haemangiomas at risk of psychosocial impact
It is difficult to determine the psychological impact of a haemangioma on a child.7 Their natural history is difficult to predict and the impact on the child is at best a subjective assessment. Consider the following aspects of psychological impact:
- Short term – parents not interacting normally with their infant despite adequate explanation.
- Medium term – many untreated haemangiomas will still be visible at 3 to 8 years of age. Psychosocial adverse effects may develop before this age, so consider early treatment of haemangiomas in cosmetically sensitive sites.
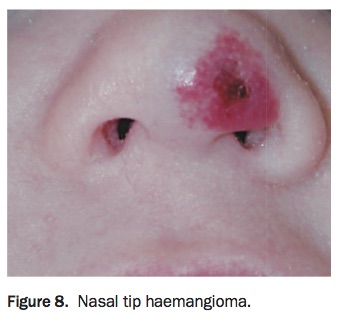
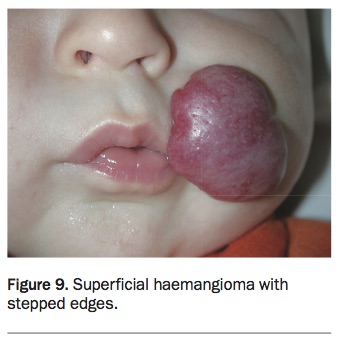
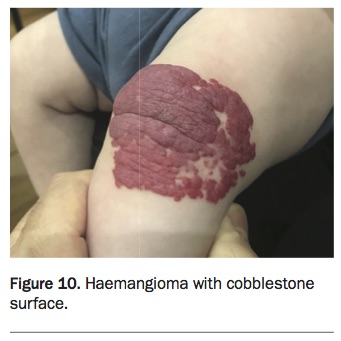
- Long term – haemangiomas can leave permanent changes including deformity, scarring, atrophy, telangiectasia and redundant skin. High-risk areas include lips (Figure 7), nose (Figure 8), cheeks and ears. Permanent nasal cartilage deformity is common with untreated nasal tip haemangiomas. Haemangiomas with a stepped edge (Figure 9) or cobble-stone surface (Figure 10) often leave permanent changes, whereas deep haemangiomas will not leave remnants.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
Oral propranolol
Since the first published report of infantile haemangioma responding to propranolol in 2008, propranolol has become the treatment of choice when systemic therapy is required.8 The exact mechanism of action of propranolol in haemangiomas has not been fully established, but it is proposed to be a complex interplay of the promotion of pericyte-mediated vasoconstriction, the inhibition of vasculogenesis and catecholamine-induced angiogenesis, the disruption of haemodynamic force-induced cell survival, and the inactivation of the renin-angiotensin system.9
Oral propranolol (or an alternative beta-blocker therapy) is the first-line therapy for infantile haemangiomas that warrant treatment and should be started and followed up in a dermatology outpatient clinic.10-12 Infants requiring treatment should be referred within weeks, not months.
Relative contraindications for propranolol
- Infants prone to hypoglycaemia: e.g. failure to thrive, concurrent/prior prednisolone therapy, poor feeding and gastroenteritis
- Cardiovascular disease, including conduction abnormalities
- Persistent bradycardia less than 100 beats per minute if child under 3 months of age, less than 90 beats per minute for children aged from 3 to 6 months
- Coarctation of aorta
- Bronchospasm
- Intracranial arterial anomalies (e.g. those seen in PHACE syndrome
- Other systemic disease.
Propranolol dosing and monitoring
In thriving, healthy infants, oral propranolol can be prescribed in an outpatient setting, and the first dose can be given at home.13,14 Start propranolol at a dose of 1 mg/kg/day (in two divided doses with food). Increase to 2 mg/kg/day after one week, unless a lower dose is clinically effective.
In smaller infants (age 0 to 4 weeks corrected and/or small for gestational age, or less than 2.5 kg body weight) and in infants with other clinical concerns (e.g. risk for hypoglycaemia) consider:
- initiation of therapy as an inpatient
- lower initial dose (e.g. 0.5 mg/kg/day)
- splitting the daily dose into three rather than two doses
- more gradual dose increases.
In higher-risk babies, consider monitoring heart rate hourly for three hours and measuring glucose three hours after the initial dose and any subsequent dose increases. Lower doses, and doses given three times a day, may also be used if clinically indicated, e.g. head/neck arterial dysplasia.
All parents should receive written instructions to cease propranolol if their child is unwell or not feeding normally. For most haemangiomas, it is acceptable to temporarily cease therapy with any significant illness, particularly if respiratory.
Monitoring propranolol treatment
For most infants, monthly review is recommended until the haemangioma shows clear signs of involution, then every three months until cessation of medication. In some settings, such as ulceration or enlarging facial lesions, more frequent initial follow up may be appropriate.
If the haemangioma is responding well, there may be no need to increase the dose of propranolol as the child’s weight increases. If the response is inadequate, consider increasing the dose of propranolol to 3 mg/kg/day (i.e. 1.5 mg/kg twice daily) and/or refer to a vascular anomalies specialist.
Ceasing propranolol treatment
The optimal treatment period with propranolol has not yet been established and may vary from three to 24 months. The aim of treatment is to switch off the proliferative phase of the haemangioma. Propranolol can be stopped safely without the need for weaning the dose. However, up to a quarter of haemangiomas will relapse after treatment is stopped.15,16 This is often minimal and temporary, but if significant, consider restarting propranolol at the previous dose.
Adverse effects of propranolol
Less serious adverse effects of propranlol are:
- sleep disturbance (wakefulness/somnolence); if persistent, consider dose adjustment or changing to atenolol (off-label use)
- cold extremities
- diarrhoea.
Serious adverse effects (uncommon) are:
- hypoglycaemic episodes/seizures
- aggravated hypoglycaemia in children, especially in the case of fasting, vomiting or overdose
- bradycardia and hypotension
- bronchospasm, e.g. during an intercurrent respiratory illness.
There is no evidence in humans that propranolol has an adverse neurocognitive effect when taken in infancy.17-21
Timing of therapy
Treat early before permanent skin changes start to develop. Treatment should ideally be started in the first weeks or months of life, preferably before or during the proliferative phase. However, it is difficult to predict which lesions will proliferate significantly.
Topical beta blocker
Treatment with a topical beta blocker (off-label use) may benefit some flat or small haemangiomas. Topical beta blockers are less effective than oral beta blockers in the treatment of infantile haemangiomas and should not replace systemic therapy in patients who have a clear indication for treatment. The most commonly used topical beta blocker is timolol maleate 0.5% gel forming drops, one drop applied to the haemangioma twice daily. Systemic absorption of topical timolol is variable but may be significant with ulcerated lesions, large lesions, or in infantile haemangiomas affecting premature or small infants.22,23
Other medical treatment
High-dose systemic steroids (2 mg/kg/day) were routinely used in the past, but are no longer considered first-line therapy. They may be considered in patients in whom oral beta blockers are contraindicated or not effective. Other treatments include oral sirolimus (rapamycin), intravenous vincristine and oral ACE inhibitors, but efficacy and safety data are limited. All are used off label.
Surgery
Most infantile haemangiomas do not warrant surgery. However, early surgical intervention, with or without oral propranolol, is considered for localised ulcerated lesions and lesions where early surgery might minimise significant psychosocial effects.
Laser
The use of vascular laser in the management of haemangiomas is limited because it can only penetrate 1 mm into the skin. Early pulsed-dye laser therapy can be of benefit in flat haemangiomas and is useful for remnant telangiectasia in mostly resolved haemangiomas in older children. Laser may also be of benefit in ulcerated haemangiomas not responding to appropriate dressings.
Conclusion
Infantile haemangiomas are very common, benign, self-limiting vascular proliferations that mostly do not require intervention. However, assessment can be difficult given the highly variable natural history of haemangiomas. Therapy is indicated in a number of circumstances and, more commonly, there are many situations in which therapy can be considered to minimise future cosmetic impact. MT