Allergic rhinitis: an update on management

Allergy
Allergic rhinitis is a common manifestation of atopy that significantly reduces quality of life. A careful history and examination, along with appropriate investigations, are needed to determine the most likely allergens and to direct treatment. Recent advances in allergen immunotherapy show promise and the ‘thunderstorm asthma’ phenomenon emphasises the need for action plans for patients with comorbid asthma.
- Allergic rhinitis creates a significant burden for affected individuals and reduces their quality of life.
- There are a broad range of differential diagnoses for allergic rhinitis, and an allergic cause for symptoms should be confirmed to direct treatment accordingly.
- There is limited evidence for the efficacy of allergen-avoidance strategies, but this may be due to the heterogeneity of the advice.
- Intranasal corticosteroids and oral antihistamines are considered first-line therapies.
- If symptoms are poorly controlled with simple strategies, referral to an allergist for possible allergen immunotherapy should be considered.
Allergic rhinitis (AR), or ‘hayfever’, is a common medical problem that can affect quality of life and restrict activities of daily living.1 Studies show a prevalence of 20 to 48% in the Australian population.2-4 AR may also involve other complications, including predisposition to upper respiratory tract infections, asthma development, sinusitis, reduced mood and cognition, school and work absenteeism, and negative impacts on speech and hearing development.5-7 It is a major risk factor for asthma. The Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines determine the severity of AR based on its frequency of symptoms (intermittent versus persistent) and impact on work, function and sleep, and show that severity of symptoms influences escalation of treatment.8,9
Typical symptoms of AR include conjunctivitis, nasal congestion, rhinorrhoea, pruritic throat and sneezing. Pollens from grasses, trees and weeds are common triggers for seasonal AR. Triggers for perennial AR include house dust mites (HDMs), cockroaches, animal dander (e.g. cat or dog) and mould. Australian studies have shown that HDMs, perennial ryegrass Timothy and, plantain and Bahia grasses are among the most common allergens to which patients are sensitised on skin prick testing (SPT), and many patients are polysensitised to allergens.10,11
AR exists on the spectrum of atopy. This includes the disorders of asthma and eczema and appears to be on the rise in both developed and developing countries.12 About one-half to two-thirds of patients with rhinitis symptoms are atopic.13,14 Although symptoms of AR are triggered by allergens, there is a separate nonallergic entity which has many causes that can be elicited by careful history, examination and investigations.15 These disorders are managed according to their aetiology but can be broadly grouped under the umbrella term of nonallergic rhinitis. Differential diagnoses to consider for patients with rhinitis symptoms are listed in the Box.
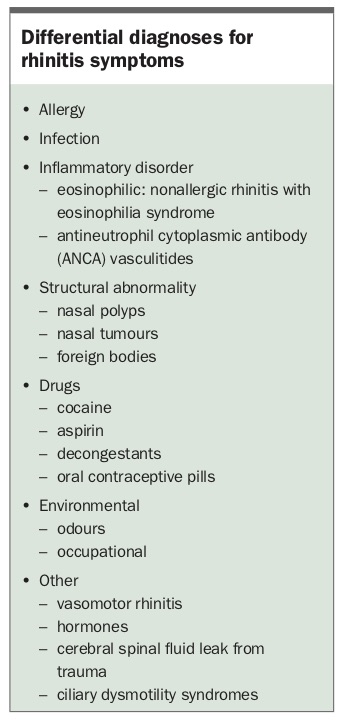{kind=link}
Investigation and diagnosis
History and examination are key to the diagnosis of AR, and investigations such as allergy SPT or allergen-specific immunoglobulin (Ig) E testing (formerly radioallergosorbent testing) are performed to support the diagnosis. Allergen-specific IgE testing is easily ordered by GPs and is particularly useful when SPT cannot be performed, such as in patients with uncontrolled asthma or when certain medications cannot be stopped. If allergy testing and history do not indicate an allergic cause for the patient’s rhinitis, the diagnosis is nonallergic rhinitis.
Children with chronic or persistent AR may display ‘allergic facies’, consisting of allergic shiners (dark rings below the eyes), nasal crease, a high-arched palate and dental malocclusion.16 Anterior rhinoscopy may show pale or boggy turbinates, as well as nasal polyps. Examination should also look for comorbid conditions, including asthma, eczema and conjunctivitis.
When ordering investigations for allergic disease, it is not advisable to use serum total IgE as a screening test for atopy. Although many patients with allergic disease do have a total serum IgE level above the normal range, a high serum-specific IgE level is still possible with a normal total serum IgE level.17 Serum-specific IgE tests should be based on the likely single allergen(s) identified on history, rather than allergen mixes, as mixed allergens are generally a screening tool and may not detect patients with low-level sensitivity. Pathology laboratories limit the number of serum-specific IgE tests that can be performed on a single sample, mandating a careful allergic history and informed assumptions about likely allergens. This will ensure that the correct allergens are ordered for serum-specific IgE testing, as well as encouraging pathology stewardship and minimising costs.
SPT is easily conducted but is not always accessible to community GPs. Although SPT has good sensitivity and specificity for diagnosing AR, it identifies sensitisation, not necessarily allergy, and the findings should correlate with the patient’s history. SPT results usually correlate with allergen-specific IgE testing, although they are not always interchangeable.18,19
For SPT, a small amount of purified allergen is introduced epidermally with a purpose-made lancet, and the wheal reaction size is read 15 minutes later. Generally, a wheal of 3 mm or larger in maximal diameter is considered a positive result. Although it correlates with serum allergen-specific IgE, the size of the wheal does not correlate with severity of disease.20 A variety of aeroallergens are available for SPT to identify possible triggers for AR symptoms.
Before performing SPT, patients need to withhold oral antihistamines and medications with antihistaminergic properties, such as tricyclic antidepressants, for a minimum of two to three days. Factors that preclude SPT include severe skin conditions (e.g. eczema), inability to withhold interfering medications and lack of patient co-operation. Poorly controlled asthma is a contraindication, as SPT may flare asthma symptoms.
CT imaging of the sinuses can complement the AR investigation, as it may identify obvious nasal anatomical defects, confirm the presence of sinus disease and detect the presence of large polyps. Patients may benefit from otolaryngological review if these abnormalities are detected. Rhinoscopy may be required to detect smaller polyps.
Management
Allergen avoidance
Although allergen avoidance appears to be an intuitive part of AR management, there is an overall lack of evidence for its effectiveness and it therefore cannot be strongly recommended in clinical practice.21 Part of the problem may be the heterogeneous nature of allergen avoidance and the fact that most allergen avoidance studies use SPT to diagnose allergy. This does not substitute for a thorough evaluation by an allergist to determine the most clinically relevant allergens and provide individualised advice for allergen control or avoidance.
HDMs are the most common cause of perennial AR. These allergens are typically found in damp places, carpets and bedding in homes, as well as in crowded public spaces.22,23 There is a plethora of HDM avoidance and control strategies, such as use of acaricides, washing of bedding in hot water and use of HDM-proof pillow covers. There is limited evidence that some of these strategies reduce allergen counts, but these carefully controlled studies show that this does not translate into clinically meaningful outcomes, often due to high HDM burden.24,25 A Cochrane review of HDM avoidance strategies identified small benefits from acaricides and bedroom environment modifications but conceded that studies so far have been small, thereby limiting definite conclusions and recommendations.26 Removal of carpets could be trialled, but there is limited evidence for its efficacy.27
In Australia, cats and, to a lesser extent, dogs are also a source of perennial allergens. Although it is often impractical to remove the animal from the house, spread of these allergens can be reduced by restricting animal access to certain rooms and by regular vacuuming (e.g. every one to two days). However, clothing may act as a fomite for bringing cat allergens into cat-free houses, and allergens may linger long after removal of the animal, making allergen avoidance particularly challenging for those with pet allergies.28 Hypoallergenic-bred animals and air filters are yet to demonstrate any significant benefit to sensitised individuals.29,30
Pollens may cause patients to be symptomatic for several months of the year or cause perennial symptoms in more tropical environments. Avoidance strategies include minimising outdoor exposure, such as gardening activities; avoiding opening house windows during the pollen season; and not hanging clothes and bedding outside on days with a high pollen count. Pollen forecasts are available on smartphone applications and websites to guide patients.
AR tends to flare on warm and windy days, when pollen is more extensively dispersed. Although rain can wash pollen away, leading to temporary relief of symptoms, it may also precipitate devastating symptoms in the context of thunderstorms, as these conditions lead to expansion and eventual rupture of pollen grains in the air. The pollen grains disperse when warm air rises and reappear at ground level during thunderstorms and sudden rainfall, leading to significant symptoms and asthma – the ‘thunderstorm asthma’ phenomenon.31 The Melbourne thunderstorm asthma event of 2016 provides a good public health lesson in identifying and preventing such occurrences by ensuring patients with diagnosed asthma have written action plans and access to inhaled bronchodilators and corticosteroids.32 In addition, patients who are pollen-sensitive should take preventive measures on high-risk days, including remaining indoors and closing windows.33
Saline irrigation
Saline irrigation (also known as nasal douching) is a simple method for bathing the nasal cavity in saline solution to remove aeroallergens, inflammatory mediators and mucus.34 It can be performed using sprays or pumps and is one of the first-line options in managing mild AR, or it can be used as an adjunct to other treatments. It is an inexpensive and simple method, although there is only weak evidence that it reduces AR-related symptoms and improves quality of life.35,36
Oral therapies
Oral antihistamines
Antihistamines are an effective first-line treatment option for those with mild-to-moderate AR. They can be classed as first-generation (e.g. promethazine, chlorpheniramine), second-generation (e.g. cetirizine, loratadine) or third-generation (active metabolites of second-generation antihistamines; e.g. fexofenadine, desloratadine, levocetirizine), and they work by inhibiting H1 antihistamine receptors. H1 antihistamines are particularly effective for treating the nasal symptoms of rhinorrhoea, nasal pruritus and sneezing.37
Second- and third-generation antihistamines do not cross the blood-brain barrier as readily as first-generation antihistamines and consequently tend to be less sedating. Concern has been raised about the adverse effects of sedating antihistamines on cognitive performance and learning, particularly in children.38 Care must be taken when using sedating antihistamines in elderly patients, due to the risks of polypharmacy and the mild anticholinergic and anti-alpha-adrenergic properties of these drugs.39
Oral decongestants
Oral decongestants include pseudoephedrine and work by vasoconstricting nasal blood vessels. As such, they are useful only for treating nasal congestion, although there are limited data supporting their efficacy for reducing symptoms of nasal congestion.40 They are generally not recommended because of concerns about their negative impacts on cardiovascular health and systemic side effects, as they can induce or worsen existing hypertension, and the possibility of rebound nasal congestion when use is abruptly ceased.41 If used, decongestants should be for short-term use only, such as in patients with acute upper respiratory infections. They are contraindicated in patients with cardiovascular disease or glaucoma.
Intranasal therapies
Topical corticosteroids
There are numerous intranasal corticosteroid (INCS) preparations, such as budesonide, mometasone, beclometasone and fluticasone, which have varying strengths. INCSs are among the most effective agents for treating persistent or moderate-to-severe AR; meta-analyses have shown them to be more effective than intranasal or oral antihistamines for reducing nasal symptoms but equal in efficacy for ocular symptoms.42
Local side effects of INCSs include epistaxis, which occurs in about 9% of patients.43 This may relate to administration technique, so instructing patients to avoid direct contact of the applicator tip to the septum and to spray laterally may mitigate this side effect. INCSs do not cause nasal atrophy or glaucoma.44
Although considered topical agents, systemic bioavailability does occur with some preparations. A meta-analysis estimated systemic bioavailability of less than 0.1% for mometasone, less than 1% for fluticasone, 34% for budesonide and 44% for beclometasone.45 Studies have nevertheless failed to identify evidence of systemic adverse effects, such as growth retardation or bone mineral density loss, with long-term use.45,46 However, caution is needed when using an INCS with high systemic bioavailability for an extended period of time, especially in children and when used with other corticosteroid therapy, such as in patients with asthma. Budesonide is generally recommended as first-line treatment for pregnant women because of its safety profile and category A rating for pregnancy.44,47
Proper technique for using intranasal sprays is paramount for optimal delivery of the medicine, and careful education of patients or their caregivers is necessary. A step-by-step guide of proper intranasal spray technique is provided as part of an AR treatment plan on the Australasian Society of Clinical Immunology and Allergy (ASCIA) website.48
Topical decongestants
Similar to oral decongestants, rapid-acting sympathomimetic nasal preparations, such as oxymetazoline and xylometazoline, provide temporary relief of nasal congestion. However, rhinitis medicamentosa precludes their long-term continuous use.
Topical antihistamines
Intranasal antihistamines, such as azelastine and levocabastine, are also popular options for managing nasal symptoms. Their popularity stems from their provision of topical and directed antihistamine control, with minimal systemic absorption and side effects. In addition, randomised controlled trials have shown intranasal antihistamines to be effective for controlling nasal symptoms and improving quality of life, compared with placebo.49 Although there are insufficient data comparing intranasal with oral antihistamines, an older study looked at intranasal azelastine compared with oral terfenadine (which has since been withdrawn from the market due to safety concerns) and found intranasal therapy was better at controlling nasal symptoms.50
Ipratropium
Ipratropium intranasal sprays work by reducing secretions and are mainly effective for treating rhinorrhoea.51 As they do not affect the histaminergic activity of AR, their use is usually reserved for patients with nonallergic rhinitis who have troubling profuse rhinorrhoea.
Mast cell inhibitors
Intranasal cromoglycates have shown efficacy in reducing nasal symptoms but are not considered as effective as other first-line therapies.52 They are available in various preparations, such as intranasal sprays and eye drops. The cromoglycates have an excellent safety profile but need to be administered multiple times a day because of their short half-life.53 Topical ocular therapies are often prescribed as add-on therapy for patients with eye symptoms that are difficult to control with an INCS or oral antihistamine and for those with vernal keratoconjunctivitis (inflammation of the conjunctiva).
Ocular therapy
Topical therapies (eye drops), including topical antihistamines, sodium cromoglycate and other mast cell stabilisers, are used for treating concurrent allergic conjunctivitis. It is important to not only control symptoms but also prevent long-term inflammation, which can damage the cornea and is difficult to treat.54 Although systemic therapy and INCSs can ameliorate ocular symptoms, some patients may elect to use eye drops if their symptoms are primarily ocular.55 A meta-analysis has provided support for the effectiveness of these agents in reducing ocular symptoms.56
Artificial tears can be used to help flush out allergens, but they are not as effective at relieving acute symptoms as rapid-acting medicated products.57 Ocular antihistamines (e.g. levocabastine) and antihistamine-mast cell stabilising agents (e.g. olopatadine) are available for relief of ocular pruritus and erythema. In one study, olopatadine eye drops were more effective than levocabastine eye drops for alleviating symptoms of allergic conjunctivitis.58 The major advantage of topical antihistamines in treating allergic conjunctivitis is their rapid onset of action and tolerability.59
Other therapies
There are combined products (e.g. an INCS plus intranasal antihistamine) that tend to perform better than either product alone or placebo.60 However, these are usually reserved for patients with moderate-to-severe AR that is not adequately controlled with a single agent.61 For severe AR, some patients have been treated with oral or intramuscular glucocorticoids, but this practice is not recommended because of the side effects of long-term glucocorticoid exposure. Referral for desensitisation therapy should be strongly considered at this stage, to avoid the long-term complications of glucocorticoid use.
Desensitisation therapy
Desensitisation therapy (often called allergen immunotherapy) in subcutaneous or sublingual form provides specific and effective treatment for the amelioration of symptoms, with substantial evidence of durable benefit. GPs play a central role in the ongoing provision and maintenance of this therapy, which is advised to last for at least three years.62 Sustained benefit can be expected for seven to nine years after discontinuation of subcutaneous desensitisation therapy, with one study showing sustained improvement in 86% of patients at six years.63,64 In the polysensitised individual, disparate immunotherapy allergen mixes (e.g. HDM and pollen extracts) should be avoided, as there is no evidence supporting this practice, and the stability of allergens is likely to be compromised.65 This mandates careful diagnosis and a clinical decision about the dominant allergen in an individual.
Sublingual desensitisation tablets are a relatively recent development in immunotherapy. They have been TGA-registered and marketed for grass pollen allergy and HDM allergy. Both these modalities have proven efficacy in appropriately selected allergic individuals with seasonal and perennial AR, respectively, over and above the benefit derived from the usual therapies described here.66,67 HDM sublingual tablet immunotherapy has also been associated with a reduction in asthma exacerbations, suggesting additional benefit in those with both AR and asthma.68 There is suggestive efficacy of the benefit of grass pollen tablet therapy in the treatment of seasonal asthma symptoms, including thunderstorm asthma.69
Subcutaneous immunotherapy carries the risk of anaphylaxis, and the injections must be administered in an appropriate clinical environment. Sublingual tablets are taken daily, at home, and cause immunomodulatory effects in a similar fashion to subcutaneous immunotherapy. They appear relatively safe to use, with scant reports of anaphylaxis, although local side effects are common.66 These are often noticed with the first dose, where significant tongue and throat itching can cause alarm. Although reports of anaphylaxis are rare, precautions such as administering the first dose under specialist observation, obligatory premedication with an antihistamine and administration only in those with no or well-controlled asthma mitigate such effects. Local side effects that can occur with daily dosing and may be troublesome in the first few weeks of use include a pruritic tongue or throat. These can best be managed by using regular antihistamines for the first few weeks of treatment. A further complication is eosinophilic oesophagitis, which can occur days to weeks after commencing therapy – this complication requires cessation of treatment.
With the recommended treatment course of about three years for both grass pollen and HDM allergens, adherence to the medication regimen and costs of therapy are challenges for patients. Immunotherapy is not subsidised by the PBS, so patients or hospitals must bear the whole cost. Sublingual immunotherapy costs about $100 per month. Regimens for grass pollen sublingual immunotherapy last from four to 12 months per year, depending on the agent prescribed. For HDM allergens, treatment is year-round, with attendant costs. Subcutaneous immunotherapy is usually less expensive, although there is limited availability of TGA-registered allergens.
An additional challenge for prescribers is that tablet immunotherapy has fixed formulations that may not be suitable for the patient’s individual allergen profile. This is especially the case for grass pollen immunotherapy in areas where subtropical grasses are thought to be a major allergen, as subtropical grasses are not included in the grass pollen tablets.70 Prescription and initiation of immunotherapy should always be managed by a physician with specific expertise in allergic disease.
Conclusion
Many nonpharmacological and pharmacological options exist to tackle troubling AR symptoms. A careful history and clinical evaluation are required to establish the most clinically relevant allergens for the polysensitised patient. This may affect allergen avoidance and choice of therapy and enables provision of individualised advice to the patient.
INCS therapies and nonsedating oral antihistamines are regarded as first-line options with good efficacy. A suggested duration for trialling treatment before review or escalation is four weeks. Available therapies are summarised in the Flowchart, which describes a suggested approach and hierarchy for the management of AR, modelled on the ARIA guidelines.8 Advantages and disadvantages of each main treatment are summarised in the Table.
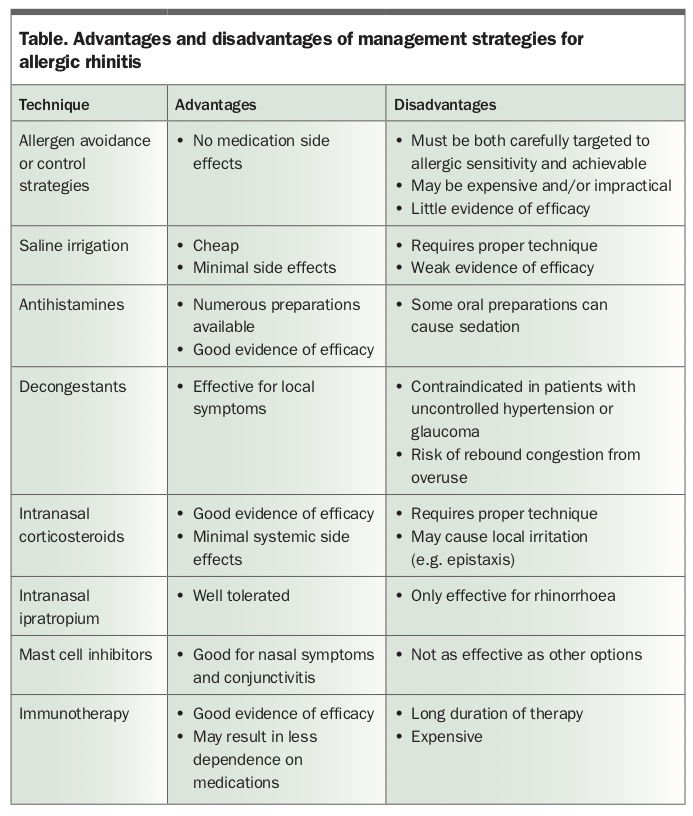{kind=link}
Ample education should be provided to patients and their families. Clarifying their expectations – that treatment is not a cure – and counselling patients about proper administration technique for medications and their side effects is crucial to optimise treatment success and patient satisfaction. The ASCIA and similar websites of other professional organisations, such as the American Academy of Allergy, Asthma & Immunology, have suitable patient handouts for educational purposes. RMT