Artificial stone: a new cause of silicosis

Lung diseases
Occupational health
Occupational silica dust exposure is one of the earliest recognised causes of lung disease. Despite this, Australia is experiencing a major outbreak of silica-related disease in workers fabricating and installing benchtops made from artificial stone.
- A major outbreak of silicosis is occurring in Australia due to the fabrication and installation of artificial stone benchtops.
- Crystalline silica is recognised as a hazardous substance under Australian law.
- Exposure to silica is also associated with tuberculosis, chronic obstructive pulmonary disease, lung cancer, scleroderma, rheumatoid arthritis and chronic renal disease.
- Urgent identification of those exposed to hazardous levels of silica due to working with artificial stone and appropriate health assessments and management are needed.
Artificial stone – a material high in silica – has become commonplace in the building and manufacturing industry over the past 20 years. But there has been a failure to recognise the risks associated with working with this material. Alarmingly, in 2018 one of the first respiratory health screening programs undertaken in two Australian stone benchtop businesses identified that one-third of the screened stonemasons had features of silicosis.1 Subsequently the Queensland Government ordered an audit of the stone benchtop industry in that state. The audit has so far revealed 98 workers with silicosis and more than 550 workplace safety breaches.2
A brief history
Silicon dioxide (silica) is the most abundant mineral in the earth’s crust. The term ‘silicosis’ was first used by Achille Visconti in 1871, however the association between silica-containing dust and lung disease dates back to Hippocrates (460 to 375 BC).3 Workers traditionally at risk of exposure were those who cut or drilled through the earth’s surface, such as miners, quarry workers and tunnellers. The Hawk’s Nest Tunnel disaster, which occurred in the early 1930s in West Virginia, resulted in silicosis being defined as a major public health issue in the USA.3 Construction of the tunnel through rock with a high silica content with minimal dust control measures resulted in at least 400 deaths and is still one of the worst industrial disasters in USA history.
Current issues
Today, problems arise when silica is introduced into nontraditional industries and occupations, and the risk is not recognised. Outbreaks of silicosis have occurred in various occupations, including dental technicians, slate pencil makers, denim jean sandblasters and, most recently, tradespeople who fabricate benchtops with artificial stone.4-7
Artificial stone (also referred to as engineered, agglomerated or reconstituted stone and quartz conglomerate) is a high silica-content material primarily used for the fabrication of household benchtops. Slabs of stone are manufactured by mixing finely crushed rock with a polymeric resin and pigments, which is then moulded into shape and heat cured.8 The silica content of artificial stone is typically more than 90%, which is much higher than that of the natural stones traditionally used to produce benchtops (on average, 3% in marble and 30% in granite).
Artificial stone was introduced into Australia in the early 2000s and since then it has become a popular choice for kitchen, bathroom and laundry benchtops. In comparison to marble, artificial stone is cheaper, stain resistant and available in a wide range of colours. By 2010, artificial stone accounted for 32% of all new benchtops fabricated in Australia, increasing to 45% in 2016.9
Australian stone benchtop businesses import slabs of artificial stone from a manufacturer. The benchtop fabricators process the slab of stone based on client specifications. They cut the slabs to the required size, create cut outs for sinks and tap wear, and then polish the final product. Commonly, workers use high-powered hand tools such as grinders. Without the appropriate regulatory contents applied, this process generates extremely high levels of very fine silica dust in the breathing zone of the worker. A 2015 study noted that cutting artificial stone without water dust suppression (dry cutting) resulted in levels of silica dust 150 times above the recommended limit of exposure for a 30-minute period.10 Even with the use of water and local exhaust ventilation during cutting, the level of silica generated was double the recommended limit, reflecting the high content of silica in the material.
The first case of silicosis associated with artificial stone was reported in Italy in 2010. Since then, the number of reports internationally has been rapidly growing.11-13 In 2015, the sentinel Australian case was a 52-year-old Vietnamese refugee who developed complicated silicosis due to extremely poor working conditions in Australia.14 Subsequently, an Australian case series described seven patients with an age range as young as 26 years (median, 44 years).7 All were involved in dry cutting; ventilation typically relied on ceiling extraction fans or passive airflow through open doors. Only three of the workers were provided with respiratory protection (usually in the form of a disposable mask). None had previously been screened for lung disease through a health surveillance program. The findings demonstrate an exceedingly poor understanding of the risk and regulations associated with working with materials with a high silica content.
Silica is recognised as a hazardous substance under Australian law and regulations require employers to maintain levels of silica below a specified exposure standard.15 If there is the likelihood that half the specified exposure standard may be exceeded, health surveillance and assessment of exposure levels must be undertaken. This is in the form of objective measurement of silica dust levels at the workplace, and lung function testing and periodic chest x-rays for workers. Despite the very high silica content of artificial stone and the clear risk of high-level silica exposure, it appears that these regulations have seldom been adhered to in the industry since its introduction in the early 21st century.
The Australian case series noted a median duration of work in the industry of seven years before onset of symptoms.7 Review of lung function results identified a rate of decline 10 times greater than the normal rate. These findings are consistent with the accelerated form of silicosis. In comparison to chronic silicosis (which develops after at least 10 years of exposure to silica), accelerated silicosis develops after five to 10 years of exposure, is associated with high-intensity exposure to silica and has a greater risk of disease progression.16
Although the level of knowledge about silicosis associated with high intensity exposure is limited, other reports also indicate a high risk of disease progression, even after cessation of exposure to silica. A Turkish study of 83 former denim jean sandblasters noted over a four-year period the prevalence of silicosis increased from 55.4% to 95.9% and radiographic progression was observed in 82%, despite no further silica dust exposure.6 These results highlight the need for ongoing monitoring of all workers identified to have had high-risk exposure to silica, including those who have left the industry.
As well as silicosis, exposure to silica is associated with other respiratory and nonrespiratory conditions, including tuberculosis, chronic obstructive pulmonary disease, lung cancer, scleroderma, rheumatoid arthritis and chronic renal disease.16,17 A study of workers with artificial stone associated silicosis referred for consideration of lung transplantation in Israel identified that 23% also had a range of autoimmune diseases, most frequently scleroderma and rheumatoid arthritis.18 Exposure to silica can also result in the development of autoimmune disease in the absence of silicosis.19
Screening, diagnosis and management
Advocacy by respiratory and occupational physicians since 2016 has resulted in a gradual increase in awareness around silicosis in the benchtop industry and, subsequently, screening of exposed workers. Urgent effort is required throughout Australia to identify those who have been exposed to hazardous levels of silica due to working with artificial stone, and to provide appropriate health assessments and management. Considering the popularity of artificial stone in this country, the number of workers who have been exposed to unsafe levels of silica is likely to be in the thousands.
Health screening must be performed at a high standard and overseen by an expert such as an occupational physician. Health screening requirements are available from the relevant state or territory government agency responsible for occupational health and safety (Box).
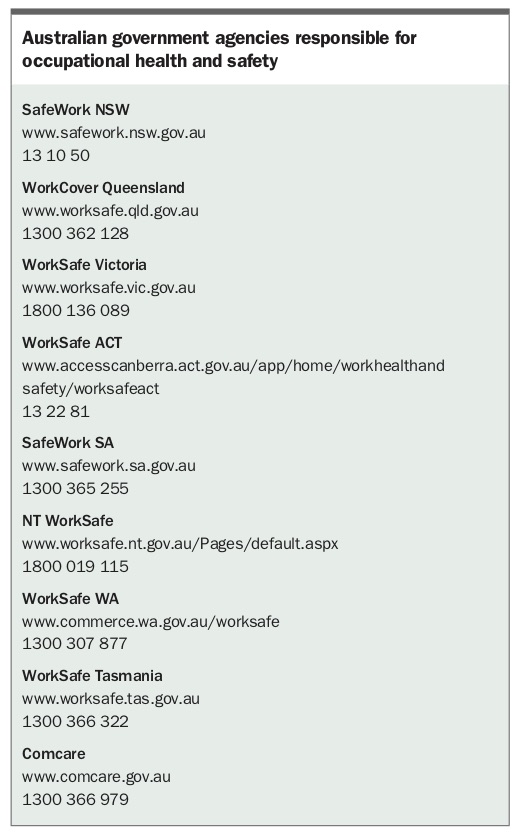{kind=link}
The diagnosis and management of silicosis can be challenging. Silicosis may be misdiagnosed as one of the other more common fibrotic lung diseases, in particular sarcoidosis. The key to identifying a possible occupational cause of lung disease, including silicosis, is to spend a few moments taking an occupational history from patients. If an occupational lung disease is suspected, or there has been occupational exposure of concern, referral to an expert respiratory or occupational physician is highly recommended.
Conclusion
Although artificial stone now accounts for about half of all new benchtops manufactured and installed in Australia, it has taken almost 20 years for regulatory agencies and many employers to recognise the risk to workers in this industry of developing silicosis. Tragically, it is highly likely that if regulation regarding occupational silica exposure had been complied with since the introduction of artificial stone to Australia, most workers would have been spared this ancient occupational lung disease.
Further information about accelerated silicosis is available from The Royal Australasian College of Physicians (www.racp.edu.au/advocacy/division-faculty-and-chapter-priorities/faculty-of-occupational-environmental-medicine/accelerated-silicosis). RMT