COPD: reducing hospitalisations this winter


COPD (chronic obstructive pulmonary disease)
Breathing problems
Effective and appropriate management of patients with chronic obstructive pulmonary disease (COPD) includes immunisation against influenza and pneumococcus, encouraging smoking cessation, regular exercise and a healthy diet, and treating exacerbations early. These measures can help prevent hospitalisations due to COPD exacerbations.
- A patient’s usual management of chronic obstructive pulmonary disease (COPD) should be reviewed in early winter, ensuring they have an appropriate treatment plan, including both pharmacological and nonpharmacological therapies.
- Pulmonary rehabilitation is an effective intervention in COPD and can improve quality of life, fitness and self-confidence, and reduce hospitalisations.
- Influenza and pneumococcal vaccinations should be kept up to date; use patient recall systems if needed.
- Patients should be encouraged to have a COPD self-management plan.
- Patients should be reviewed early and regularly after an exacerbation, whether they are treated at home or in hospital; readmission risk is highest within three months of discharge.
- The involvement of outreach and community home services in the management of patients with COPD should be considered.
- Early treatment of patients with exacerbations of COPD may reduce hospitalisations.
Chronic obstructive pulmonary disease (COPD) is currently the fifth leading cause of death in Australia with many deaths occurring as a result of an exacerbation.1 COPD is a common clinical problem encountered in general practice, with about one million Australians being significantly affected by long-term lung conditions characterised by shortness of breath, such as chronic bronchitis and emphysema.2 Exacerbations of COPD can significantly impair a patient’s quality of life, contribute to progressive decline in lung function and are frequently under-recognised by both the patient and medical staff. A considerable increase in the number of COPD exacerbations and hospital admissions is seen during the winter months, and deaths from COPD tend to be highest in the late winter months (July to August).3
This article reviews current recommendations for the care of patients with COPD and the management of exacerbations in the general practice setting, with the aim of reducing the number of exacerbations and hospitalisations this winter. Advanced treatment measures for exacerbations of COPD are beyond the scope of this review and are not discussed in detail here.
What is COPD in 2019?
Our understanding of COPD has evolved dramatically over the past two decades, with the past 10 years in particular seeing an exponential increase in research in COPD. Successful new options for treatment have been developed and new evidence has informed the use of older drugs in certain types of patients with COPD. There has been a shift from an airflow limitation (forced expiratory volume in one second [FEV1]) and ‘one size fits all’ approach to diagnosis and management towards recognition of COPD as a very complex and heterogeneous condition. This recognition is leading to increased individualisation of COPD management.4
International guidelines from the Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommend that COPD be considered as a whole condition, not just by the degree of airflow obstruction.5 Severity of airflow limitation (based on postbronchodilator FEV1) remains a core feature, but symptoms experienced by the patient and history of moderate or severe exacerbations should now be included in the assessment. Dyspnoea is a better prognostic indicator of mortality in COPD than FEV1, and previous history of exacerbations is the best surrogate marker of the risk of future exacerbations.
Precision medicine is defined as ‘treatments targeted to the needs of individual patients on the basis of genetic, biomarker, phenotypic or psychosocial characteristics that distinguish a given patient from other patients with similar clinical presentations’.6 The ultimate aim of precision, or individualised, medicine is to provide the most appropriate treatment for individual patients while avoiding unnecessary medications and minimising side effects. COPD is well suited to an individualised medicine approach because it likely represents not a single disease but a continuum of different diseases that may share biological mechanisms and present similar clinical features, but which have varying treatment responses.
A patient’s phenotype is composed of traits or characteristics produced by the interaction between their genes and the environment.7 Some of these traits will be amenable to treatment, others will not. COPD phenotypes were traditionally defined as chronic bronchitis (‘blue bloater’) and emphysema (‘pink puffer’). In the past the limited alternatives for pharmacological treatment made it unnecessary to clinically identify different types of patients. However, the number of treatments now available for COPD treatment has increased considerably over the past decades. Phenotyping can help clinicians identify patients who share clinical characteristics and outcomes and, more importantly, similar responses to existing treatments. It has become increasingly evident that not all patients respond equally to all drugs, and the need to identify ‘responders’ is crucial.
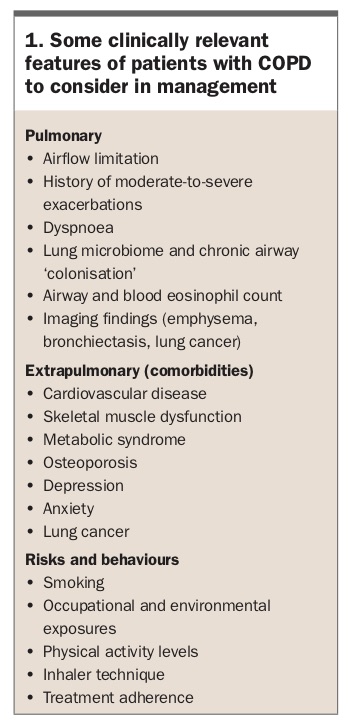
There is no consensus on the definition and number of different COPD phenotypes, which may be anywhere from two to 328 million (estimated worldwide number of patients with COPD in 2010).8 Some clinically relevant COPD phenotypes include:8
- ‘frequent exacerbators’ with two or more exacerbations per year, who may benefit from anti-inflammatory treatment added to bronchodilators
- ‘overlap COPD-asthma’ who have an enhanced response to inhaled corticosteroids
- ‘infrequent exacerbators’ whose treatment may be based on long-acting bronchodilators, either alone or in combination; and
- high rates of ‘comorbidities’, particularly cardiovascular disease and metabolic syndrome, who may benefit from aggressive risk-factor management (Box 1).
{kind=link}
Who is at risk of COPD?
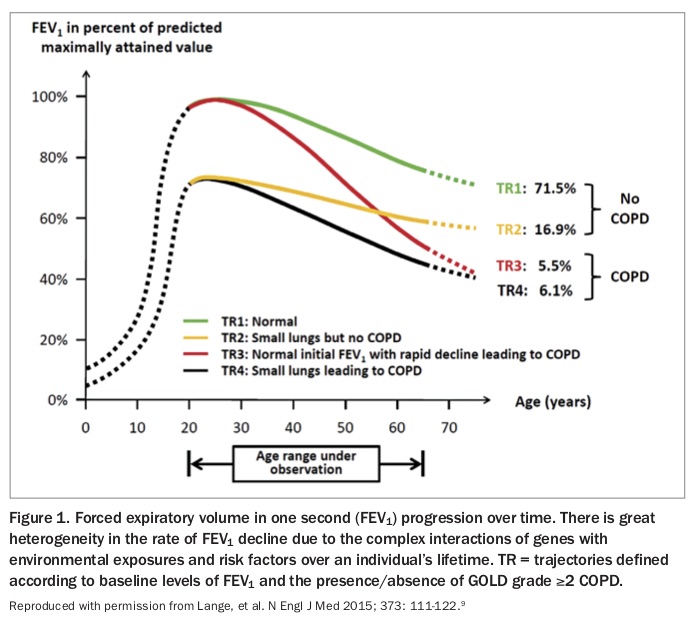
Tobacco smoking remains the major risk factor for COPD. However, even among heavy smokers, fewer than 50% develop clinically significant COPD, and some genuinely light smokers or nonsmokers develop chronic airflow limitation.5 Genetics, lung growth and development, asthma and other environmental exposures are some of the factors that can lead to an individual developing COPD in later life. COPD is generally thought to result from an accelerated decline in FEV1 over time, but in some patients it may be related to reaching early adulthood with a low FEV1 due to impaired lung development during neonatal, childhood or adolescent periods (Figure 1).9
{kind=link}
COPD should be considered in any patient who has dyspnoea, chronic cough or sputum production, and a history of exposure to risk factors for the disease, mainly smoking (usually more than 10 to 15 pack years). Measurement of FEV1 by spirometry remains the diagnostic test for COPD and should be performed in all patients with suspected COPD. COPD is defined as a postbronchodilator FEV1 to forced vital capacity (FVC) ratio of below 0.7.10 If the airflow obstruction is fully reversible, the patient should be treated as for asthma.10
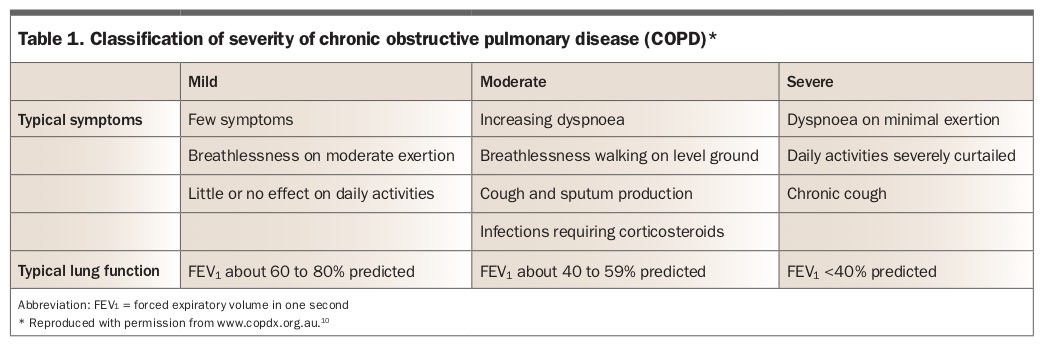
Under-recognition and underdiagnosis of COPD remain prevalent. However, patients with a history of smoking and symptoms suggestive of COPD need thorough assessment; the problem may be COPD alone, but often symptoms are due to a combination of cardiovascular disease, deconditioning and other issues, as well as airways disease. There is a continuum of COPD from mild to severe disease. Severity of airflow obstruction and the patient’s symptoms are taken into account. One classification, from the COPD-X guidelines, is shown in Table 1.10
{kind=link}
Who is at risk of a COPD exacerbation?
All patients with COPD may develop exacerbations, and even those with underlying mild disease may experience a severe exacerbation, particularly in the winter months. Those with severe COPD are more likely to have a serious outcome even with a mild exacerbation. The single best predictor of exacerbations is previous exacerbations, across all levels of COPD severity. However, exacerbations also become more frequent as COPD severity worsens.
The lung ‘microbiome’ is likely to be one of the factors involved in exacerbation risk; the more pathogens present in the lower airways, the worse the COPD outcome. Patients with COPD may have lower airways colonised by bacteria including Haemophilus influenzae, Streptococcus pneumoniae and Moraxella catarrhalis. Pseudomonas aeruginosa and Staphylococcus aureus may colonise airways of patients with severe airflow obstruction, and appear associated with more frequent exacerbations and worse outcomes. Identification of these patients may highlight a higher exacerbation risk (and also direct antibiotic management when needed). Other causes of exacerbations include left ventricular failure, pulmonary embolus and urban air pollutants.
Exacerbations may be triggered by respiratory tract infections, either viral or bacterial. In a recent retrospective study in Australian hospitals, the most common viruses isolated in patients presenting with COPD exacerbations were influenza virus, rhinovirus and respiratory syncytial virus A/B.11 Patients who do not receive influenza vaccination are at higher risk.
Optimising baseline COPD management
Ensuring that each patient’s usual COPD management is effective and appropriate will help in reducing both exacerbations and the impact of exacerbations. The Australian and New Zealand COPD guidelines are regularly updated. The current version is available online through the Lung Foundation Australia website (https://copdx.org.au).10 These guidelines are known as the COPD-X plan, from:
C – confirm diagnosis
O – optimise function
P – prevent deterioration
D – develop a self-management plan and manage
X – exacerbations.
An approach to the management of patients with COPD based on these guidelines is discussed in this article.
Referral of patients
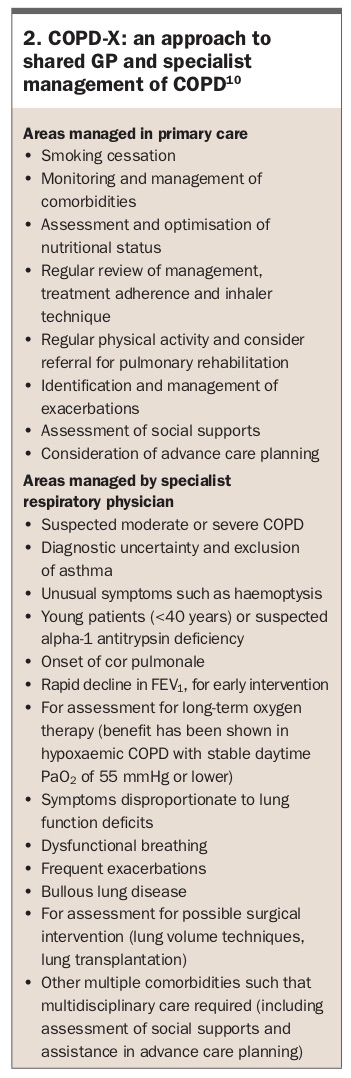
Referral of patients to a respiratory physician should be considered if their COPD is moderate to severe, the diagnosis is unclear or complications such as cor pulmonale are present (Box 2).10
{kind=link}
Treatment
Management strategies in patients with COPD focus on the relief of symptoms, the prevention of disease progression, and the prevention and treatment of exacerbations and complications, with the aims of improving exercise tolerance and health status, and reducing mortality. The extents to which these goals can be realised vary with each patient, and some treatments will produce benefits in more than one area. Treatments include both pharmacological and nonpharmacological therapies.
In addition, patients with COPD are often elderly and frequently have comorbidities such as cardiac failure, diabetes and gastro- oesophageal reflux disease. These issues may be worsened by COPD medications, and the comorbidities themselves may aggravate symptoms of COPD such as dyspnoea. Osteoporosis risk should be specifically assessed as it is common in this patient group, and may be worsened by corticosteroid use.
Pharmacological therapy
There has been an increase in the types and numbers of inhaler devices and medications available for COPD maintenance therapy, which has caused confusion in some specialists, GPs and patients alike. However, the classes of inhaled medications have not changed: short-acting beta2-agonists (SABA), long-acting beta2-agonists (LABA), short-acting muscarinic antagonists (SAMA), long-acting muscarinic antagonists (LAMA) and inhaled corticosteroids (ICS). Within these classes of inhaled medications, many options are now available; however, meta-analyses to date have not shown any statistically significant differences among LAMAs in preventing moderate-to-severe exacerbations of COPD.10 Comparisons within other classes appear limited at present.
When considering treatment for an individual patient, factors to consider include the patient’s symptoms, COPD severity and comorbidities, and the type of inhaler device to use. Combining two medications of the same class, such as a LABA/LAMA or LABA/ICS combination and an additional LABA is not advised; the risk of side effects is increased for no added symptomatic improvement.
Inhaler technique is often suboptimal, including in those who are long-term inhaler users. Use of multiple inhaler device types is associated with an increase in errors and may be associated with a poorer outcome in patients with COPD. Therefore, frequent review of inhaler technique and rationalisation of device type is beneficial.12,13
SABA and SAMA
Short-acting bronchodilators, such as the SABA salbutamol or the SAMA ipratropium bromide, can be used as as-needed therapy for patients with only occasional dyspnoea. SABAs can be given for immediate relief of symptoms in patients already using a long-acting bronchodilator for maintenance therapy. SABAs and SAMAs can improve lung function and dyspnoea. Side effects are generally minor; however, a meta-analysis of randomised controlled trials, and a later cohort study, found an increased risk of adverse cardiovascular events with ipratropium bromide.14 This has not been seen with tiotropium.15,16
LAMA, LABA and LAMA/LABA combinations
Patients who need more than occasional use of short-acting bronchodilators may be started on a single long-acting bronchodilator, either a LAMA or LABA. A recent meta-analysis comparing LABAs with LAMAs assessed 16 randomised double-blinded controlled trials of patients with moderate-to-very-severe COPD.17 It found that LAMAs were associated with a lower risk of acute exacerbations and lower incidence of adverse events, compared with LABAs. No significant differences between LAMAs and LABAs were found in terms of changes in lung function, symptoms or health status. LAMAs may be preferable to LABAs in patients with stable COPD, especially those at risk of frequent exacerbations.17
In patients with persistent dyspnoea on one bronchodilator treatment, a second bronchodilator should be added.5 Several LAMA/LABA fixed-dose combinations delivered in a single inhaler are available in Australia, via a range of devices. A network meta-analysis of LAMA/LABA combinations compared with the individual monotherapies found that the fixed-dose combinations provided benefits in lung function and quality of life, with no increase in adverse outcomes.18 Combination therapy reduced moderate-to-severe exacerbations compared with a LABA alone but not compared with a LAMA alone. Effects on severe exacerbations were similar with both combination and monotherapies. Other network meta-analyses have also found benefits for LAMA/LABA fixed-dose combinations, compared with their monocomponents.19 PBS requirements for these medications should be taken into consideration.
Inhaled corticosteroids
There is ongoing debate about the role of ICS in patients with COPD. The potential benefits of ICS must be balanced against the potential risks including local oropharyngeal adverse effects and pneumonia. A meta-analysis of 43 studies of COPD showed an increased risk of pneumonia with ICS use, but this was balanced against the benefit of reduced exacerbations.20 Their main impact is to reduce the risk of exacerbations; in contrast to long-acting bronchodilators their effects on symptoms and lung function are small and often insufficient to use as a guide to treatment efficacy.
Treatment with ICS is directed at patients deemed to be at risk of exacerbations because of a past history of exacerbations and/or poor lung function.21 There is emerging evidence that blood eosinophil counts may be a useful biomarker of ICS response in patients with COPD.22 Those with blood eosinophil counts less than 100 cells/mcL appear less likely to benefit from ICS, and those with a count of more than 300 cells/mcL are more likely to benefit. ICS inhalers alone are not indicated for COPD; the combination of an ICS and a LABA is used in COPD as this works better than an ICS inhaler alone.
A reasonable approach based on current evidence is to consider the addition of ICS to long-term maintenance bronchodilator therapy in patients with COPD and a history of multiple or severe exacerbations and poor lung function (FEV1 <50% predicted), particularly if blood eosinophil counts are more than 300 cells/mcL, and in those with COPD and asthma. The risk of pneumonia is higher in patients of older age, with a lower body mass index (BMI), with greater general fragility and who are receiving higher ICS doses, and possibly in those with blood eosinophil counts less than 100 cells/mcL.22 Patients should be educated that if they develop a chest infection they should receive antibiotic treatment promptly. Comorbidities, especially osteoporosis and diabetes mellitus, should also be taken into account.
In general, the use of drugs in COPD does not involve back titration. The exception is when oral corticosteroids have been given for an exacerbation. Additionally, in light of recent trials, in patients with COPD with no evidence of asthma and with infrequent exacerbations ICS withdrawal can be considered.10 Close monitoring is advised after withdrawal, and withdrawal should be considered cautiously in those with elevated blood eosinophil counts and/or poor lung function.
Other therapies
Long-term use of systemic corticosteroids is not recommended in patients with COPD due to an unfavourable risk-benefit ratio.10 However, short-term use to treat exacerbations is supported by good-quality evidence, with reduction in the severity of exacerbations, shortened recovery times and reduced hospital admissions and readmissions being noted.10
Several recent trials of monoclonal antibodies targeting interleukin-5 to reduce eosinophil activity have suggested that biologic therapies may have value in the treatment of patients with COPD and eosinophilia.23 Further prospective trials are awaited. Phosphodiesterase type-4 inhibitors are potential candidates for the treatment of COPD, but this class of medications is currently not available in Australia.
Several trials have suggested that in patients with moderate-to-severe COPD and frequent exacerbations, long-term treatment with oral macrolides may reduce the frequency of exacerbations. However, owing to the potential significant adverse effects including cardiac toxicity, ototoxicity, diarrhoea and antibiotic resistance it is recommended that specialist advice be sought if this therapy is being considered.24 There is no evidence base to support long-term use of other antibiotics.
Theophylline has a modest bronchodilator effect, but is not currently recommended in Australia. This is because of its narrow therapeutic index, its potential for significant side effects and the lack of demonstration of a reduction in exacerbation rates in patients who are on adequate inhaled therapy.25
Nonpharmacological therapies
Smoking cessation
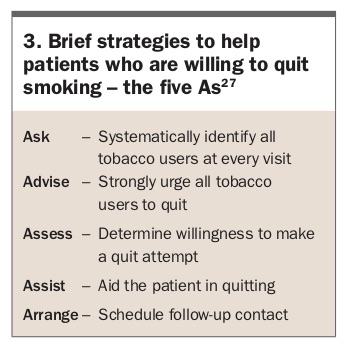
Smoking cessation remains the single most effective intervention to slow the progression of COPD. Short-term benefits on lung function and quality of life are also seen. GPs should aim to identify all current, or relapsed, smokers at every consultation as each brief counselling intervention increases the chance of successful cessation by 5 to 10%.26 No single cessation plan works for all; a discussion is needed with each patient to find the best technique. As few smokers are successful in their first attempt at quitting, persistence by everyone is important. Smoking cessation is usually a long-term process rather than a single event, with episodes of relapse before long-term success is achieved. The five As can be used as a framework for helping patients to quit smoking (Box 3 and Box 4).27
{kind=link}
{kind=link}
Nicotine dependence is most effectively treated with a combination of nicotine replacement therapy (NRT), behavioural support and pharmacotherapy. NRT (available as a patch, gum, lozenge, sublingual tablet and inhaler) is widely available, and more than one form of NRT can be used concurrently with increased success rates and no safety risks. All forms of NRT monotherapy can increase the rate of quitting by 50 to 70%. Higher-dose forms of NRT (4 mg) are more effective than lower-dose forms (2 mg) for more addicted smokers.
Varenicline is a nicotinic receptor partial agonist that more than doubles the chances of quitting compared with placebo. Adverse effects include unusual mood change, depression, behaviour disturbance and suicidal thoughts. A Cochrane review found that varenicline helped about 50% more people to quit than nicotine patches and ‘other’ forms of NRT (tablets, sprays, lozenges and inhalers), and about 70% more people than nicotine gum.28 Combining two types of NRT was as effective as using varenicline, and helped more people to quit than single types of NRT.
Bupropion, a non-nicotine oral therapy, significantly increases cessation rates compared with placebo. It has been shown to be effective for smokers with depression, cardiac disease and respiratory diseases, including COPD. A recent Cochrane review found evidence that smokers with COPD who received a combination of high-intensity behavioural support and medication were more than twice as likely to quit as people who received behavioural support alone. It found no clear evidence that one particular form of behavioural support or medication is better than another.29
Immunisations
Influenza immunisation can reduce the incidence of serious illness and death in patients with COPD, and a significant reduction in the number of exacerbations has been seen in immunised patients.5,10 All patients with COPD should be offered annual influenza vaccination. Development of an immune response takes at least two weeks. The protective efficacy of the vaccine is largely determined by the closeness of the match between the circulating influenza virus strains and the vaccine, and will vary from year to year. One multicentre study suggested that influenza vaccine efficacy decreases in older adults as frailty increases.30 Despite this, a recent meta-analysis suggested that older adults receiving influenza vaccination may have a lower risk of influenza and lower respiratory tract infections than those not vaccinated.31 Repeat vaccination later in the influenza season may also be considered in the elderly and in those with underlying severe airways disease.
Previously, a history of anaphylaxis or a serious allergic reaction to eggs was an absolute contraindication to influenza vaccination. However, several studies now suggest that most people with an egg allergy, including anaphylaxis, can safely receive influenza vaccines that contain less than 1 mcg of ovalbumin per dose.32 Review of the guidelines of the Australasian Society of Clinical Immunology and Allergy and specialist opinion should be considered in these patients. Influenza vaccine should not be given to patients with a current febrile illness or history of Guillain-Barré syndrome.
Pneumococcal immunisation is recommended for all patients with COPD. People with COPD vaccinated with injectable polyvalent pneumococcal vaccines are less likely to experience an exacerbation of COPD or episode of community-acquired pneumonia. At present, the 23-valent pneumococcal polysaccharide vaccine (23vPPV) given twice five years apart is recommended for adults aged 65 years and over. Expert opinion is divided about whether to continue to recommend 23vPPV or to replace its use with the more effective 13-valent pneumococcal conjugate vaccine (13vPCV). One small randomised, controlled trial found a significant additive effect of receiving both vaccines on exacerbations in patients with COPD.10
Physical activity and reducing sedentary behaviour
On average, people with COPD participate in 57% of the total duration of physical activity undertaken by healthy controls.33 Reductions in physical activity commence early in COPD and, over time, levels of physical activity substantially decline across all severities of COPD. This decline is accompanied by a deterioration in lung function and health status.34 Levels of physical activity are reduced further during hospitalisation for a COPD exacerbation. Recovery back to previous levels of activity often does not occur.
Low levels of physical activity are associated with increased mortality and exacerbations in people with COPD.35 Regular physical activity is recommended for all individuals with COPD. People with COPD should be encouraged to be physically active and participate in activities of daily living that require the use of muscle strength, such as lifting or gardening as well as doing physical activities they enjoy, such as bowls, golf or swimming.10
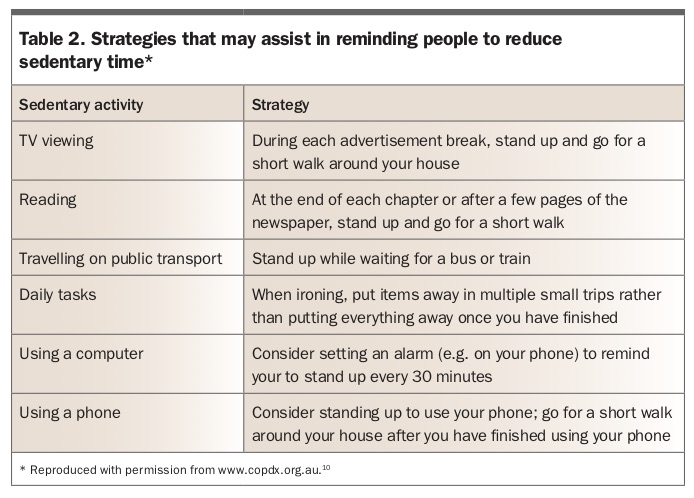
In addition to low levels of physical activity, there is growing recognition that people with COPD spend many of their waking hours in sedentary behaviours, defined as those behaviours that are undertaken in a sitting or reclined posture and have low energy requirements, such as watching television, reading and sitting at a computer. People with COPD with the greatest sedentary time during daily life are characterised by more frequent exacerbations, lower exercise capacity, long-term oxygen use, lower motivation for exercise and the presence of physical comorbidities including obesity and arthritis. Compared with the goal of increasing moderate- or high-intensity physical activity, the goal of reducing sedentary time by increasing light-intensity physical activity is likely to be more feasible in some patients with COPD. Of note, in people with COPD, greater participation in light-intensity physical activity has been reported to reduce the risk of respiratory-related hospitalisations.36 Table 2 provides some strategies aimed at avoiding prolonged sedentary time.10
{kind=link}
Pulmonary rehabilitation
The benefits of pulmonary rehabilitation in improving dyspnoea, quality of life, exercise capacity, anxiety and depression, fatigue and emotional function are well established. Evidence also suggests that pulmonary rehabilitation is safe and highly effective in reducing hospital admissions and mortality and improving health-related quality of life in COPD patients after exacerbations.10
Pulmonary rehabilitation programs consist of general assessment of the patient and specific assessment of exercise capacity and quality of life, followed by an exercise program and education sessions. Pulmonary rehabilitation programs are available at many community centres and hospitals, and usually welcome referrals from GPs.
Nutrition
Both obesity and low BMI are associated with increased morbidity in patients with COPD. Obesity increases the work of breathing and is associated with sleep apnoea, hypoventilation and cor pulmonale, as well as metabolic complications. Malnutrition is an independent predictor of mortality and use of healthcare services in patients with COPD. Energy intake is often reduced due to dyspnoea, medications and lung hyperinflation whereas expenditure is increased due to the metabolic demands of breathing, infections and systemic inflammation. Low BMI and low fat-free mass are inversely associated with respiratory and peripheral muscle function, exercise capacity and health status. Importantly, those with poor nutrition are most likely to benefit from nutrition therapy before an under-nutrition state is established.37 Nutritional supplementation in malnourished patients can improve walking distance and respiratory muscle strength. High-calorie nutritional supplements should be considered in patients with COPD and a low BMI, particularly those who are malnourished and/or have severe disease.
Self-management and action plans
COPD self-management programs may lead to improved health-related quality of life, with reduced exacerbations being a positive outcome of some studies. Other studies have not shown benefit. Trials to date have used a wide range of study designs and interventions, thus no recommendations as to the essential elements of a COPD self-management program can be made.10
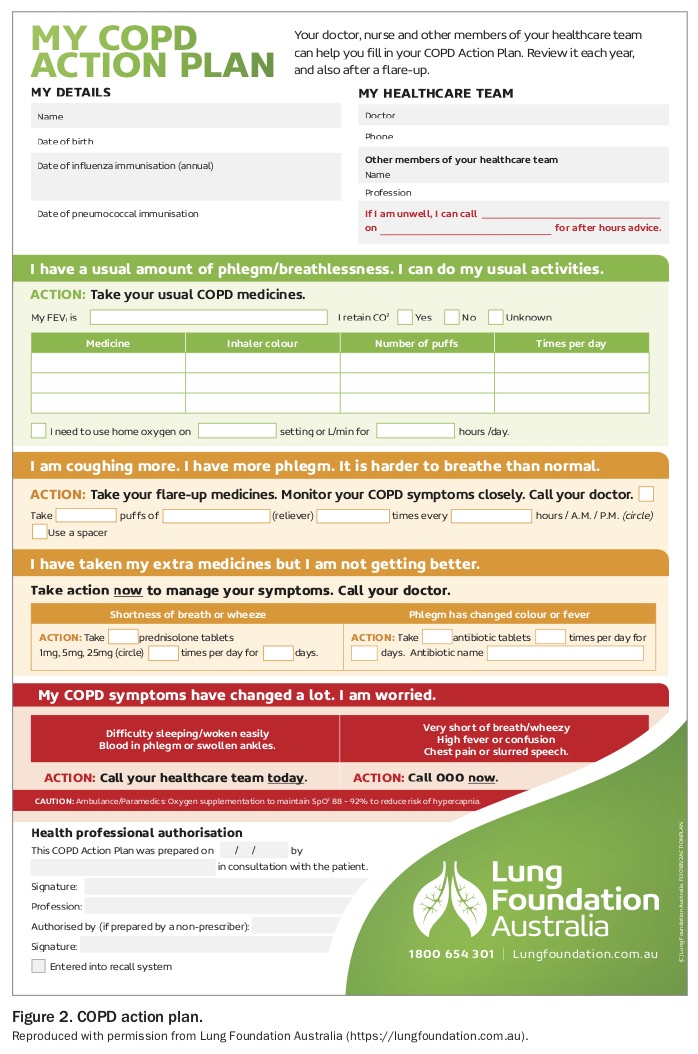
Interventions targeting mental health, an active lifestyle, relaxation therapy, use of action plans, correct medication use and facilitated access to services have been found to reduce exacerbations and visits to the emergency department. Written action plans have been shown to reduce emergency department visits and hospital admissions. Action plans should be completed by the clinician and patient together, with the aim of assisting the patient to identify symptoms of an exacerbation and know what actions they should take. A sample action plan is shown in Figure 2.
{kind=link}
Anxiety and depression are common in patients with COPD and are associated with reduced quality of life, poor self-management and medical symptoms. There is also some evidence that mood disorders are independent risk factors for exacerbations and hospitalisations. Elderly patients with COPD prescribed benzodiazepines may be at increased risk of exacerbations; caution with use of these medications, or avoidance, is warranted in all patients with COPD due to their potential for depression of respiratory drive. Behavioural therapy and selective serotonin receptor inhibitors (SSRIs) may be better management options, along with referral to clinical psychologists and psychiatrists.
In patients with debilitating breathlessness despite optimal COPD management, referral for specialist advice, consideration of judicious use of low-dose opiates and palliative care involvement can be considered. Use of a handheld fan can also be of considerable help
Outreach teams
Many regions now have specialist multidisciplinary outreach teams to assist in the co-ordination of home care. For example, in Victoria, the Hospital Admission Risk Program aims to reduce avoidable hospital admissions and emergency department presentations (www.health.vic.gov.au/harp-cdm).
Services provided by these teams may include outreach services with rapid response such as a mobile assessment and treatment service (assessment by medical practitioner and outreach nurse) and home visit assessment service. Other home services, such as physiotherapy and pharmacy, may also be accessible. The evidence is not yet available for the overall patient and economic benefits of home care, but a systematic review of seven studies found no significant differences in readmission rates or mortality, and ‘Hospital at Home’ schemes were preferred by patients and carers.38 Some patients may need initial hospital assessment, and may then be able to return to their own homes with increased social support and a supervised medical care package.
Prompt treatment of exacerbations
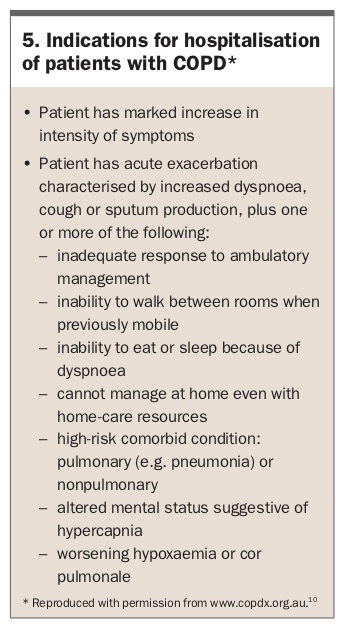
Early identification of a COPD exacerbation and early primary care management may reduce the need for hospitalisation. Initial management includes use of short-acting bronchodilators, oral corticosteroids and/or antibiotics. Indications for hospitalisation of patients with a COPD exacerbation are shown in Box 5.
{kind=link}
Follow up after hospitalisation
All patients discharged from hospital after an exacerbation of COPD should have an early (preferably within one week) follow-up consultation with their GP. The risk of readmission is highest within three months of discharge, and more than half of patients are readmitted within 12 months. All the preventive strategies for COPD exacerbations discussed above should be revisited during this consultation, including revising the patient’s COPD self-management or action plan. Pulmonary rehabilitation has been shown to reduce readmissions if provided within one week.39
This may also be an appropriate time to discuss advance care directives with patients and, if appropriate, their family and carers. End-of-life issues are relevant for patients with severe and moderate COPD; most patients with end-stage COPD wish to participate in end-of-life management decisions and would prefer to do so in a nonacute setting. For some patients, palliative care team involvement can be helpful.
Conclusion
To help reduce the number of hospitalisations due to COPD exacerbations in the colder winter months, GPs should ensure that their patient’s usual COPD management is effective and appropriate. They can also encourage their patients to be vaccinated against influenza and pneumococcus, avoid exposure to cigarette smoking, participate in regular exercise and have a healthy diet and good nutritional state. Educating patients with COPD to pay particular attention to their respiratory symptoms, follow their self-management plan, seek early treatment for any decline in their condition and avoid exposure to other people with coughs and colds will also help reduce their risk of a severe exacerbation.
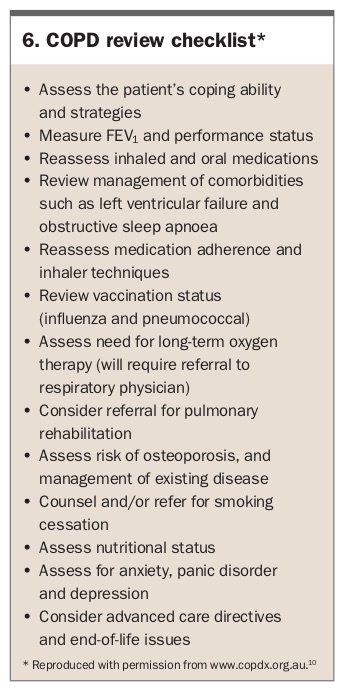
A checklist of the strategies recommended when reviewing patients with COPD is given in Box 6. RMT
{kind=link}