Pneumococcal disease and vaccination recommendations. The state of play


Bacterial infections
Overall large reductions in cases of the severe form of pneumococcal disease have been achieved with the pneumococcal vaccination program targeting all infants and older adults and individuals with risk conditions. However, uptake of vaccination recommendations targeting groups with risk conditions and Indigenous adults is suboptimal, and currently a disproportionate burden of pneumococcal disease is borne by these people. Ensuring these individuals receive the full schedule of recommended vaccine doses on time is crucial.
- Pneumococcal disease is a collection of clinical manifestations that includes life-threatening meningitis, pneumonia and septicaemia caused by Streptococcus pneumoniae.
- 13-valent pneumococcal conjugate vaccine (13vPCV; Prevenar 13) and 23-valent pneumococcal polysaccharide vaccine (23vPPV; Pneumovax 23) are offered under the National Immunisation Program (NIP) and recommendations for their use differ by target population.
- The recent change in the recommended schedule for 13vPCV for infants to include a 12-month age booster dose after primary doses at age 2 and 4 months is expected to prolong protection for vaccinated children as well as improve herd benefit for others.
- For individuals with underlying medical conditions that increase their risk of pneumococcal infection there are targeted vaccine recommendations and vaccine providers need to ensure that all such people are identified and given the full course of the recommended pneumococcal vaccines on time.
- A dose of 23vPPV is recommended and fully funded under the NIP for Indigenous adults at 50 years of age and non-Indigenous adults at 65 years of age.
Pneumococcal disease is a collection of clinical manifestations caused by Streptococcus pneumoniae (also called pneumococcus). In studies of the global disease burden of pneumococcal disease in children published in both 2009 and 2018, about 11% of all deaths among children under 5 years of age were reported to be attributable to pneumococcal infection.1,2 Invasive pneumococcal disease (IPD) is the severe end of the pneumococcal disease spectrum. In IPD, S. pneumoniae is detected in normally sterile sites such as blood and cerebrospinal, pleural, pericardial, peritoneal or joint fluid.3 IPD causes significant mortality and morbidity in children, particularly among young infants. In developed countries, IPD commonly (about 70% of cases) presents in children as bacteraemia with no identifiable specific focus of infection.4,5Among adults, the most common presentation of IPD is bacteraemic pneumonia.6,7 Noninvasive pneumococcal disease, which is localised mucosal infections of S. pneumoniae, is generally less serious and more common than IPD. Among pneumococcal disease manifestations that are noninvasive, acute otitis media is the most common in children.8 Also, most cases of community-acquired pneumonia (CAP) caused by pneumococci among adults are noninvasive.9
Bacteriology of pneumococcal disease
S. pneumoniae is an encapsulated Gram-positive coccus. The polysaccharide capsule is the important virulence factor.3,10,11 Currently, about 97 pneumococcal serotypes belonging to about 40 serogroups have been identified.12,13 Serotypes differ in the chemical composition of their polysaccharide capsules and are therefore immunologically distinct.14,15 In most cases, S. pneumoniae resides in the nasopharynx leading to stable asymptomatic colonisation (carriage), which is a precursor to disease and plays an important role in horizontal transmission between individuals.16 High pneumococcal carriage seen in young children acts as the main reservoir for disease in older adults.16,17 Pneumococcal serotypes vary in their tendency to cause asymptomatic carriage or disease, and a limited number of serotypes are responsible for pneumococcal disease.14,16,18-20 Vaccines target the serotypes that commonly cause disease.
Pneumococcal vaccines available in Australia
Two types of pneumococcal vaccines have been developed and used against pneumococcal disease: pneumococcal polysaccharide vaccines (PPVs) and pneumococcal conjugate vaccines (PCVs).21-23 PCVs comprise a selected number of pneumococcal polysaccharides conjugated to a protein carrier.24,25 PPVs generate protective antibodies against pneumococcal disease without involving T cells, which are required for long-term immune memory.13 As a result, immunity triggered by PPVs is relatively short lived, and they are less immunogenic in children under 2 years of age. The covalent coupling to the protein carrier in PCVs converts the pneumococcus polysaccharide to a T cell-dependent antigen, thereby inducing immune memory and enhancing the antibody response.21 PCVs are therefore able to elicit robust, high-quality immune responses sufficient to prevent pneumococcal disease even in very young infants.
There are two pneumococcal vaccines available in Australia through the National Immunisation Program (NIP):
- Prevenar 13 (Pfizer), 13-valent pneumococcal conjugate vaccine (13vPCV).
- Pneumovax 23 (Seqirus/Merck), 23-valent pneumococcal polysaccharide vaccine (23vPPV).
Recommendations of the Australian Technical Advisory Group on Immunisation (ATAGI) regarding the use of pneumococcal vaccines are published in the Australian immunisation handbook (https://immunisationhandbook.health.gov.au).26 These recommendations regarding which vaccine to use and the required number of doses and timing are based on the different characteristics of the vaccines and a person’s individual risk of IPD. An individual’s risk of IPD varies by:
- age
- Indigenous status
- state/territory of residence
- the presence and nature of risk factors, including both immunocompromising and nonimmunocompromising underlying medical and selected behavioural conditions
- previous doses of pneumococcal vaccines received.
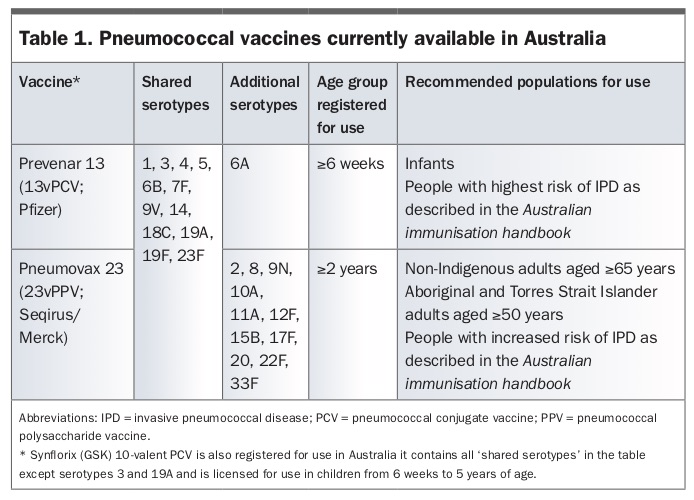
Table 1 summarises important details regarding pneumococcal vaccines currently available in Australia.
{kind=link}
Most of the ATAGI-recommended pneumococcal vaccine doses are fully funded by the government under the NIP, and for some recommendations the vaccine cost is subsidised under the PBS. People occasionally have to pay the full cost of the vaccine.
Risk factors for pneumococcal disease
Certain medical and lifestyle conditions are associated with increased risk of pneumococcal infection as well as more severe disease outcomes across populations . After they were licensed, pneumococcal vaccines were offered to those population groups at high risk of IPD; the specific recommendations for additional vaccine doses for those groups are still in place but compliance seems poor. Studies have shown that pneumococcal vaccines led to a decline in IPD caused by serotypes targeted by the vaccines in some of these groups, but the decline is less than that observed among people with no such risk conditions (risk factors).27,28 As a result, in this post-PCV era a large proportion of pneumococcal disease in children and adults is in those with risk factors. Individuals with risk factors are susceptible to disease caused by a broader range of pneumococcal serotypes than those with no risk factors.29,30 The use of 23vPPV is recommended for these people to account for this.
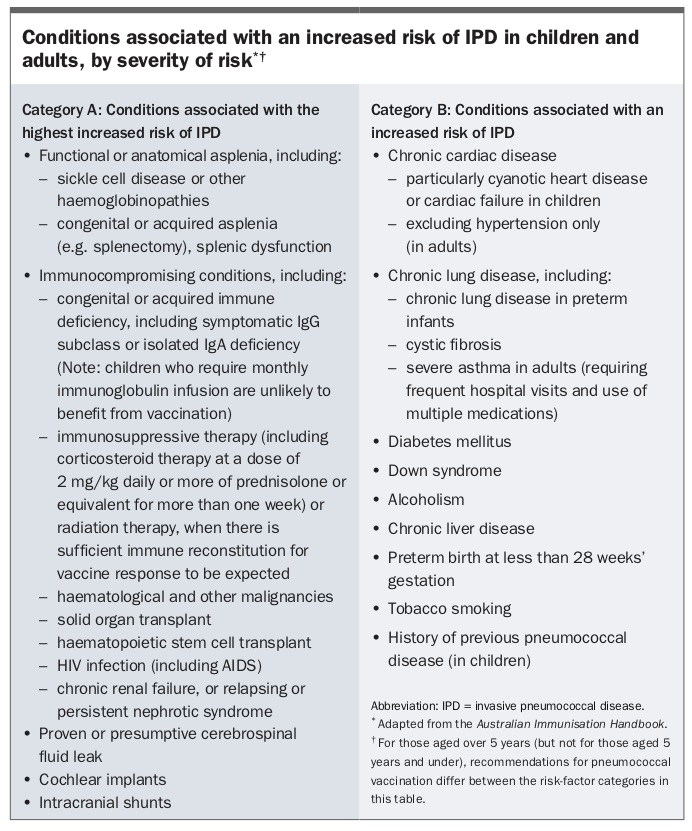
The magnitude of the increased risk of pneumococcal disease varies quite considerably by individual risk conditions. People who are unable to mount an adequate immune response to pneumococcal capsular antigens because of immunocompromised states caused by disease or therapy are at particularly high risk of IPD, some as much as up to 100 times greater than those with no risk conditions.3,31,32 Several studies have reported HIV infection and immunosuppressive therapy (e.g. after solid organ transplantation) as major factors associated with increased susceptibility to IPD.28,33-37 Other chronic diseases shown in these studies as strong risk factors for IPD include bronchial asthma, renal disease, chronic airway disease and diabetes mellitus.28,38 In addition, the incidence of pneumococcal disease is substantially higher among those with inherited conditions such as sickle cell disease and primary immunodeficiencies.27,39,40 There are also other chronic medical conditions that are important risk factors for IPD.41 In the Australian immunisation handbook the conditions for which risk factor-based pneumococcal vaccination recommendations apply are grouped into categories A and B based on their associated level of risk, and for that reason the recommendations vary between the two categories (Box).26
{kind=link}
The incidence of IPD among Indigenous Australians is currently higher than that among non-Indigenous Australians for all age groups. Since the introduction of funded pneumococcal vaccination in early 2000, the IPD burden for Indigenous Australians has only decreased among children directly targeted for vaccination.42 Among Indigenous adults, including young adults, the total IPD incidence has increased, in contrast to that in the non-Indigenous population, in which substantial reductions were seen across all ages due to direct as well as good indirect (herd) impact of the childhood vaccination program. As a result, in the last decade or so the disparity of IPD incidence between Indigenous Australians and non-Indigenous Australians has widened. Currently, the lowest incidence of IPD among Indigenous adult age groups is in the 15 to 24 years age group and is comparable with the incidence among non-Indigenous adults aged 65 years and over.
Pneumococcal disease epidemiology in Australia
IPD has been a nationally notifiable disease in Australia since 2001. The National Notifiable Disease Surveillance System (NNDSS) captures all notifications of IPD in the country. In 2018 there were 2032 cases of IPD notified to NNDSS with, as in other years, episodes peaking in the winter months.43 There were 131 deaths in that year reported as being due to IPD, most among elderly adults. The incidence of IPD is highest in extremes of age, with about 18 per 100,000 population in children under 2 years of age and 25 per 100,000 population in adults aged over 85 years.44
In the 10 years after the rollout through the NIP of funded pneumococcal vaccination in 2005 for all children and older adults, the IPD incidence among all Australians halved.45 The decline of more than 80% in young children was particularly remarkable. The pneumococcal disease incidence among Indigenous Australians is several-fold higher than for non-Indigenous Australians. Of all IPD cases in 2018, 11% were in Indigenous people, who make up about 3% of the Australian population.43
Unlike for IPD, there are limited data available on the epidemiology of noninvasive pneumococcal disease. Among Australian adults aged 65 years and over, about 45,000 are hospitalised because of pneumonia annually. Of these, about 6300 (14%) have pneumococcal CAP. A further 1400 patients with pneumococcal CAP are managed by GPs.46,47
Among Australian children, the two PCVs that have been used in the universal infant pneumococcal vaccination program, 7vPCV and 13vPCV, are highly efficacious. The three-dose schedule of both vaccines had more than 90% effectiveness in children against IPD caused by serotypes they contained.48,49 These vaccine effectiveness assessments showed that without a booster dose vaccine-induced immunity waned when children reach their second year of life.49,50 This led to ATAGI revising the schedule for 13vPCV by moving the third dose given at 6 months of age to be a booster dose at 12 months of age to prolong immunity. The PCV programs also led to large declines in IPD caused by vaccine serotypes in unvaccinated older children and adults, mediated through reduction in asymptomatic carriage of pneumococcus in vaccinated children. The 23vPPV vaccine offered to older adults had 61% effectiveness against IPD caused by serotypes covered in that vaccine in Australian adults aged 65 years and over.51 In recent IPD notifications data, about 40% of cases in children under 5 years of age were caused by 13vPCV serotypes.43
Current pneumococcal vaccination strategy in Australia
The Australian immunisation handbook digital version contains the current ATAGI recommendations for pneumococcal vaccination.26 They are summarised below according to age and risk-factor status. The ATAGI recommendations differ in some ways from the manufacturers’ product information. Previous anaphylaxis with vaccine or components is an absolute contraindication to vaccination.
For children without risk factors
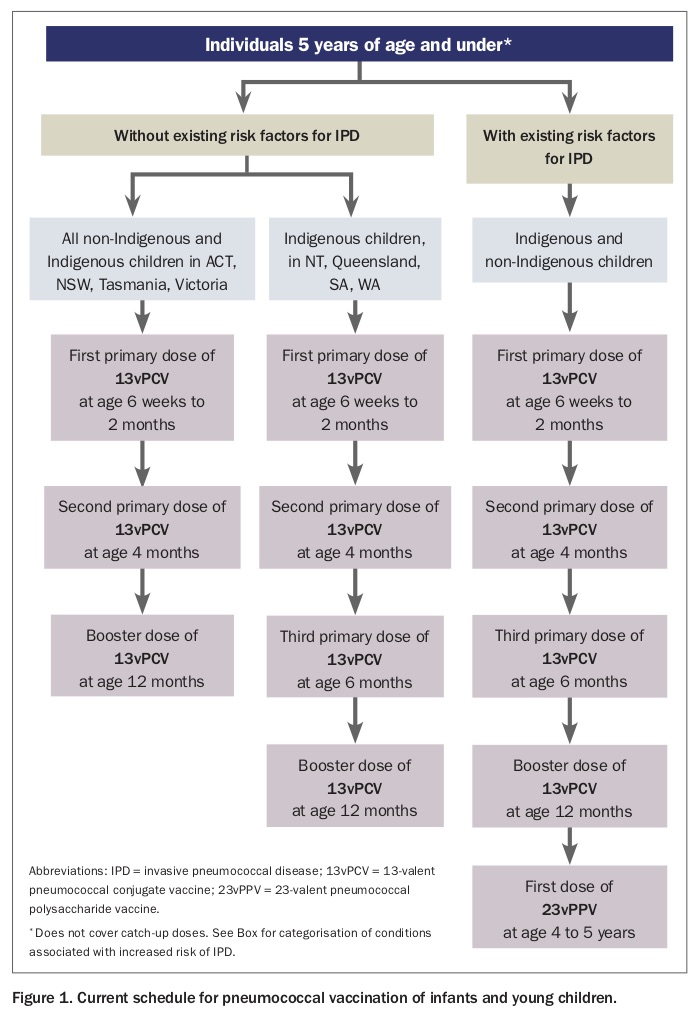
For all non-Indigenous children and Indigenous children in the ACT, NSW, Tasmania or Victoria without any of the risk factors listed in the Australian immunisation handbook (Box), three doses of 13vPCV at ages 2 months, 4 months and 12 months (2+1 schedule) are recommended and funded (Figure 1). It is also recommended that the first dose can be given at 6 weeks of age, at the same time as the first dose of pertussis-containing vaccine. Those infants should still receive their next scheduled dose at age 4 months. Before 1 July 2018, the schedule recommended for these children was three primary doses at ages 2, 4 and 6 months. The third primary dose was then moved to become a booster dose in order to make vaccine-induced protection last longer. During the transition period, it was recommended that children who had already received three doses of 13vPCV who reached the age of 12 months after 1 July 2018 also receive the booster dose at 12 months of age. Having this booster dose in the 13vPCV schedule is expected to also substantially improve herd protection.
{kind=link}
For Indigenous children living in the NT, Queensland, SA and WA, a booster dose of 13vPCV after three primary doses at 2months, 4 months and 6 months of age is recommended and funded (3+1 schedule). This booster dose was previously given at age 12 months in SA and 18 months in NT, Queensland and WA. The recommended schedule point for the 13vPCV booster for all eligible children from 1 July 2018 onwards is 12 months of age.
For children who have a delayed start to their vaccination and for those missing doses, the schedule to follow depends on their age at presentation; the Australian immunisation handbook stipulates the number and timing of 13vPCV doses in these scenarios. No pneumococcal vaccine doses are recommended for children after 5 years of age unless they have underlying risk conditions, owing to the otherwise relatively low risk of pneumococcal disease.
For older adults without risk factors
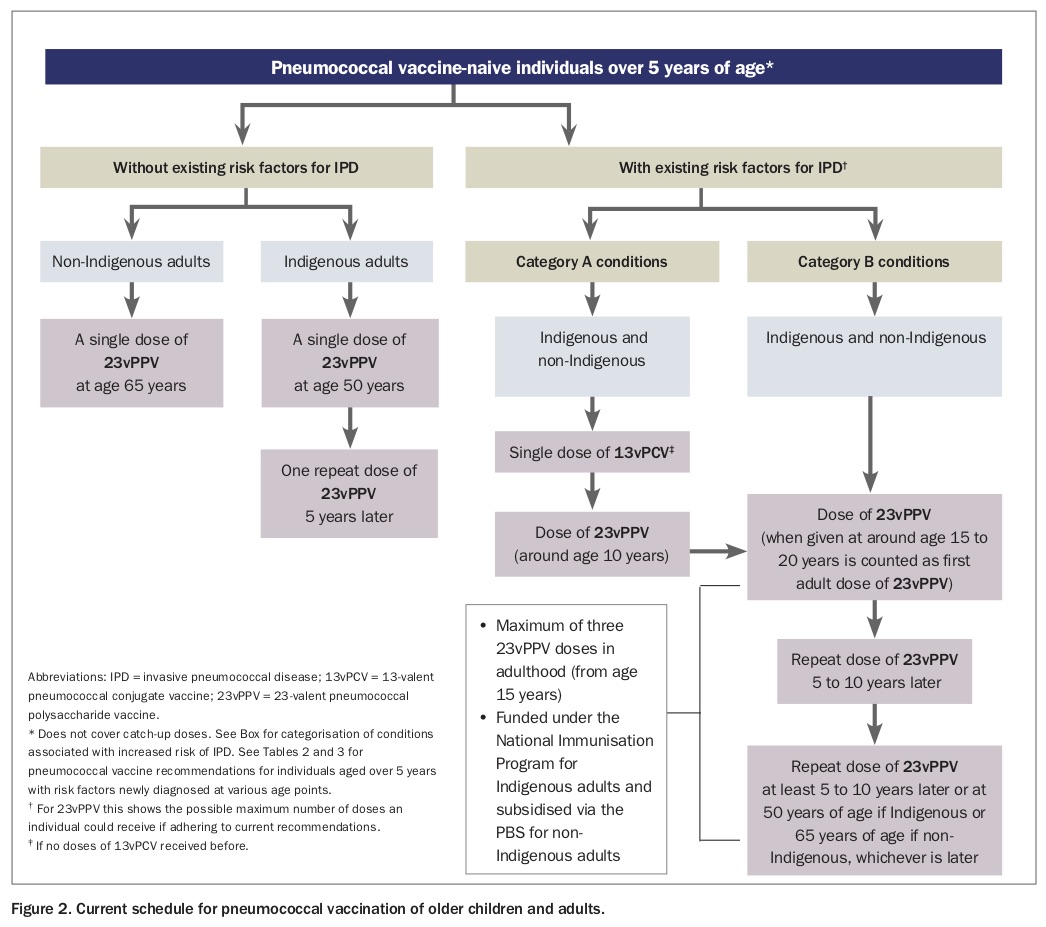
A dose of 23vPPV is recommended and fully funded under the NIP for Indigenous adults at 50 years of age and non-Indigenous adults at 65 years of age (Figure 2). These people are still eligible to receive the funded 23vPPV at any age if they have not been vaccinated when reaching these scheduled ages. For older Indigenous adults only, a second dose of 23vPPV is recommended and funded five years after the previous dose. Before 2011 a second 23vPPV dose was recommended for non-Indigenous older adults also, but due to the high rates of local reaction – including some severe injection-site adverse events – ATAGI decided to discontinue the recommendations for a repeat 23vPPV dose except for those with increased risk of pneumococcal disease.
{kind=link}
For people with risk factors listed in the Box
For children with underlying medical risk factors (both category A and B), three primary doses of 13vPCV at age 2, 4 and 6 months followed by a booster dose at 12 months of age (i.e. 3+1 schedule) are recommended and funded (Figure 1). After the course of 13vPCV, children with medical risk factors are also funded to receive a dose of 23vPPV at 4 to 5 years of age.
It is recommended that children with a category A risk factor receive a second dose of 23vPPV about five years after the previous 23vPPV dose (i.e. at about 10 years of age) followed by another 23vPPV about 10 years after the previous dose or at about 18 to 20 years of age, whichever is later.
For all individuals who undergo allogeneic or autologous haematopoietic stem cell transplant, three doses of 13vPCV followed by a dose of 23vPPV are recommended regardless of previous pneumococcal vaccines received. The three doses of 13vPCV are to be given six, eight and 12 months after transplant and the 23vPPV dose 12 months after the last 13vPCV dose.
The recommendation for children with category B risk factors is to give the second dose of 23vPPV about 10 years after the first dose that was given at 4 to 5 years of age (i.e. at age 15 to 18 years).
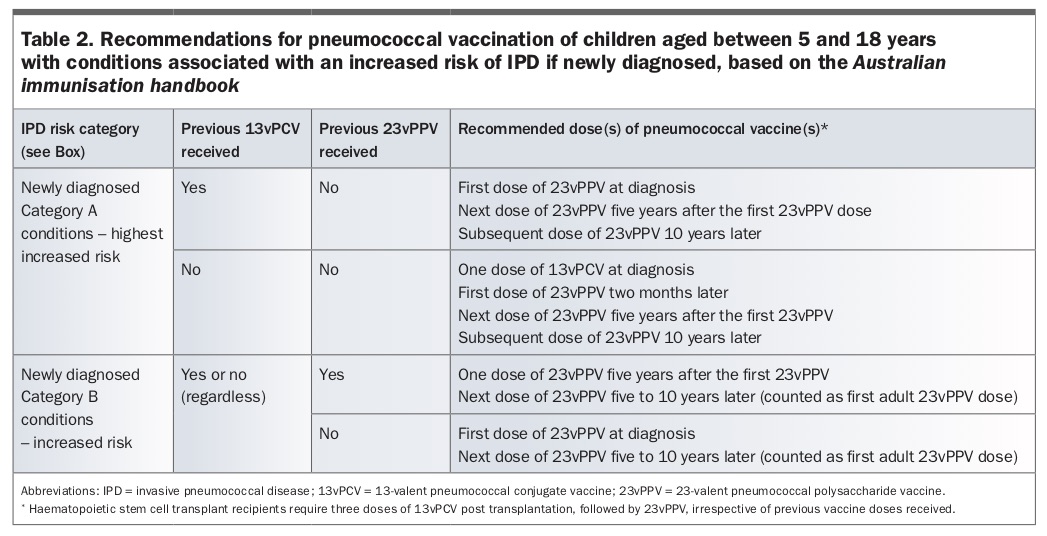
People may be diagnosed with these risk factors at different ages. The schedule to follow varies according to the age, whether the person is Indigenous or non-Indigenous, their risk factor category (A or B) and what pneumococcal vaccines, if any, they have received already. Table 2 summarises the recommendations for those who have risk factors diagnosed between the ages of 5 and 18 years. Of note, if the person has a category A risk factor then a dose of 13vPCV is to be offered if it has not been given previously. Thereafter, 23vPPV is to be given at the specified intervals.
{kind=link}
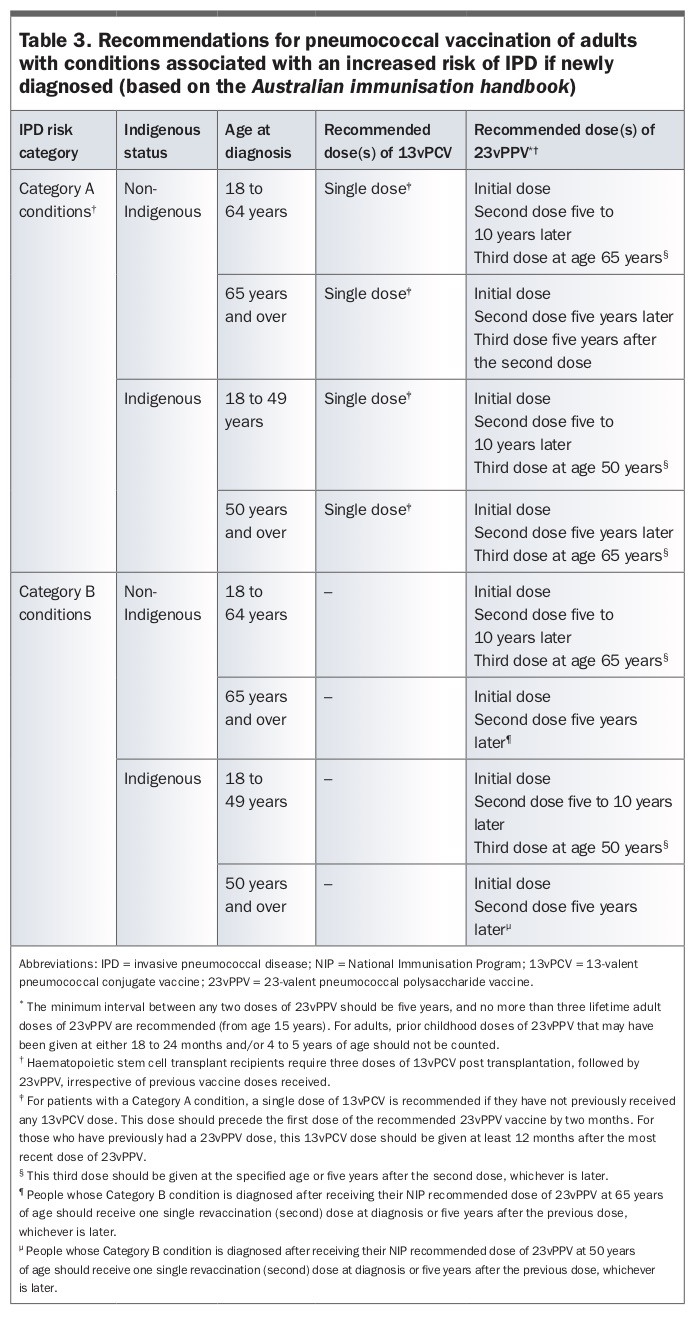
It is recommended that all adults (Indigenous and non-Indigenous) aged 18 years or over who have risk conditions (either category A or B) receive up to three lifetime doses of 23vPPV (Figure 2 and Table 3). For adults with Category A risk factors a single dose of 13vPCV is recommended if they have not previously received any dose of 13vPCV, although this is not currently subsidised. If the person has received a dose of 23vPPV previously, the recommended interval before the 13vPCV dose is 12 months. Thereafter, a dose of 23vPPV is recommended after an interval of at least two months and at least five years since the last dose of 23vPPV. The next 23vPPV dose is recommended at about five to 10 years (minimum five years) after the previous 23vPPV dose. For Indigenous adults the third and final dose of 23vPPV is recommended at age 50 years or at least five years after the second dose (whichever is later). For non-Indigenous adults, the third and final dose of 23vPPV is recommended at 65 years of age or at least five years after the second dose (whichever is later).
{kind=link}
If adults with category A risk conditions present for their first pneumococcal vaccination at or after 50 years of age, if Indigenous, and 65 years of age, if non-Indigenous, a dose of 13vPCV followed by up to three doses of 23vPPV vaccine are to be given conforming to the intervals described above. For Indigenous adults the third dose is to be given at a minimum of 65 years of age. If the adult has a category B risk factor then two doses of 23vPPV are recommended.
Conclusion
The pneumococcal vaccination program targeting all infants and older adults and individuals with risk conditions led to large reductions in the severe form of pneumococcal disease overall. However, currently a disproportionate burden of pneumococcal disease is borne by Indigenous adults and people with risk conditions. Although there are vaccination recommendations specifically targeting groups at high risk, it is likely that uptake is suboptimal. The susceptibility of these high risk groups to disease caused by a broader range of pneumococcal serotypes compounds the problem. Recent changes to the infant 13vPCV schedule will lead to longer-lasting protection in vaccinated children and better herd effect, benefitting all. Vaccine providers need to particularly focus on ensuring that all people with risk conditions are identified and given the full course of recommended pneumococcal vaccine doses. RMT