Aspirin-exacerbated respiratory disease. More than just sensitivity to aspirin

Breathing problems
A 43-year-old man with aspirin-exacerbated respiratory disease (AERD) is under consideration for aspirin desensitisation. His asthma is currently uncontrolled with moderately severe airflow limitation and he is likely to have poor adherence. Aspirin desensitisation is a possible treatment option, but would it be safe at this stage?
- Every patient with asthma should be asked if they experience nasal or respiratory symptoms after taking aspirin or other NSAIDs.
- About 8% of patients with asthma and 15% of patients with severe asthma have aspirin-exacerbated respiratory disease (AERD).
- Diagnosis of AERD is based on the symptom triad of asthma (often adult-onset and severe) and nasal polyposis plus a respiratory and/or nasal reaction to taking an NSAID.
- If the history of reactions is not clear, formal aspirin challenge under carefully controlled conditions is the current standard for diagnosis. Severe bronchospasm may occur.
- If asthma and nasal symptoms are inadequately controlled with standard medical and surgical therapies aspirin desensitisation and daily aspirin treatment is an option in patients with AERD.
- Other add-on options include leukotriene receptor antagonists or biologic agents for severe asthma.
Case scenario
Mark is a 43-year-old man with a longstanding history of nasal trouble and allergies. He reports having allergies as a child and remembers having dark rings around his eyes, but he was a sprinter throughout his school years and had no symptoms of asthma during childhood and adolescence. In his late 20s he developed back pain, for which he took aspirin. This provoked severe wheeze and shortness of breath that required monitoring in a local emergency department. He had a subsequent less severe reaction to ibuprofen, and has avoided both aspirin and ibuprofen ever since.
Mark developed nasal polyposis soon after this time and first underwent surgery for this at the age of 30 years. His most recent surgery was six months ago. Mark has daily symptoms of asthma (chest tightness and shortness of breath) and tends to wake once a week with symptoms. He attributes all of these symptoms to postnasal drip with green mucus, which is present daily. He can breathe through his nose and can taste and smell without problems except when he has an infection. His asthma triggers include exercise (for example, running with his children), colds, some foods (wine, wheat, dried apricots) and exposure to bleach and Palmolive soap. He is allergic to cats.
He was prescribed a high dose combination fluticasone propionate/salmeterol metered dose inhaler (250/25 mcg two inhalations, twice daily) but relies on inhaled salbutamol twice daily and nebulised salbutamol twice weekly to carry out his activities of daily living. He uses nasal saline rinses with budesonide infrequently, preferring to swim to clear his nose. He took oral corticosteroids around the time of his most recent nasal surgery but has not used oral corticosteroids apart from this. He has never seen a respiratory physician and was referred by his ear, nose and throat surgeon to the immunology clinic for consideration of aspirin desensitisation to help improve his recurrent nasal polyposis.
Mark works in property maintenance, is a nonsmoker and no longer drinks alcohol. He lives in a home unit with his wife and his two children who are 3 and 6 years of age.
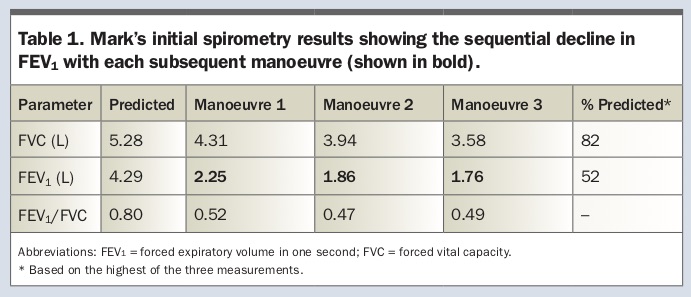
On examination at the immunology clinic, there was an audible wheeze. There was no inflammation in the throat and no visible polyps in the nose. Examination of the chest after salbutamol administration revealed widespread expiratory rhonchi with occasional inspiratory rhonchi. Spirometry performed before salbutamol administration revealed sequential bronchoconstriction with each subsequent manoeuvre (Table 1). After the testing he became very wheezy and required nebulised salbutamol 5 mg.
{kind=link}
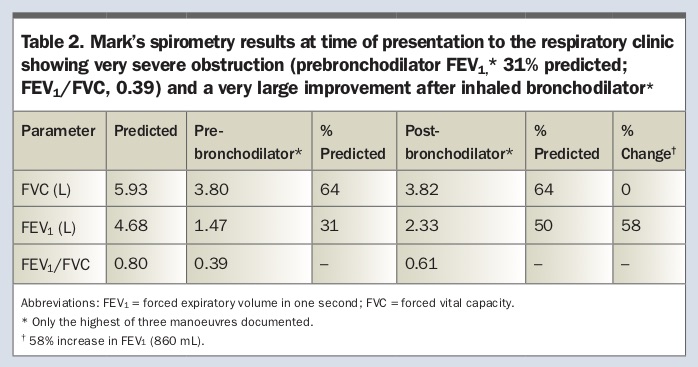
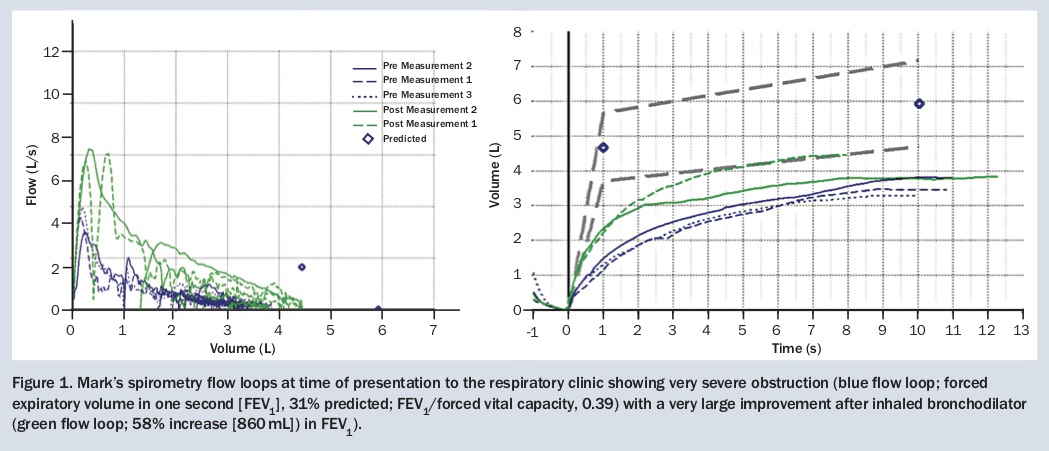
During Mark’s immunology clinic appointment, the importance of taking his prescribed inhaled corticosteroid/long-acting beta-2 agonist (ICS/LABA) inhaler regularly was stressed. He was referred to the asthma clinic, and was seen there a few weeks later. Spirometry at this review showed very severe airflow limitation with only partial reversibility (Table 2, Figure 1), with results as follow:
{kind=link}
{kind=link}
- forced expiratory volume in one second (FEV1) before salbutamol administration, 1.47 L (31% predicted)
- FEV1 after two puffs of salbutamol 2.33 L (50% predicted; an increase of 58%)
- forced vital capacity (FVC) before salbutamol administration, 3.8 L (64% predicted)
- no change in FVC after salbutamol.
Should Mark go ahead with aspirin desensitisation? What should be done before desensitisation?
Commentary
In summary, Mark has AERD with Samter’s triad of asthma, nasal polyposis and aspirin sensitivity. His asthma is currently uncontrolled with severe airflow limitation and he is persistently poorly adherent with asthma treatment. He is likely to have severe airway hyper-responsiveness. In this context, aspirin desensitisation would be dangerous at this stage.
There are several red flags in Mark’s history. The first is his frequent requirement for inhaled short-acting beta agonist (salbutamol) to treat his regular day- and night-time symptoms of breathlessness. This should instantly provoke questions about his adherence and his inhaler technique with the prescribed ICS/LABA preventer (fluticasone propionate/salmeterol). On further questioning, it emerged that, despite the counselling provided at the immunology clinic, Mark had continued to under use his ICS/LABA inhaler, taking it ‘only when his breathing gets bad’, and then he will take it at most once a day for a few weeks. Recently he had been taking about three puffs of his ICS/LABA a week (i.e. about 10% adherence).
Mark sees his main problem as being with his nose. He has very poor adherence to all his respiratory and nasal medications, and forgets to take them as he is busy with his business and family and does not see his asthma as a high priority. He also admits that he is ‘not keen’ on taking medications.
The second red flag is that his spirometry results at the immunology clinic (Table 1) showed sequential bronchoconstriction with each subsequent manoeuvre. Loss of the usual bronchodilator effect with deep inspiration is seen in asthma, and it may be reversed among patients with severe or uncontrolled asthma.1 It indicates that Mark likely has very severe airway hyper-responsiveness and thus he is at very high risk of severe exacerbation.
The third red-flag is his poor perception of airflow limitation, as indicated by the presence of few symptoms on the day of the asthma clinic consultation despite FEV1 of only 31% predicted. Impaired perception increases his risk of a severe or life-threatening exacerbation.
Aspirin-exacerbated respiratory disease and Samter’s triad
AERD usually includes the triad of asthma, chronic rhinosinusitis with nasal polyposis and an acute reaction to aspirin (acetylsalicylic acid) and other cyclo-oxygenase (COX)-1-inhibiting NSAIDs. The reaction classically involves symptoms in both the upper respiratory tract (nasal congestion, frontal headache or sinus pain and sneezing) and the lower respiratory tract (cough, wheezing, chest tightness) occurring 20 minutes to three hours after drug ingestion.
The estimated prevalence of AERD is about 7.2% among patients with a diagnosis of asthma, and is twice as high (14.9%) among patients with severe asthma.2 It is 9.7% among patients with nasal polyps and 8.7% among those with chronic sinusitis.2
The three components of AERD develop serially over years, as with Mark, and AERD is usually diagnosed in adulthood.3 Most patients develop rhinitis initially, which is usually established by their 30s, followed by chronic rhinosinusitis with the development of nasal polyposis. As the rhinosinusitis worsens, inflammation develops in the lower respiratory tract and the patient is diagnosed with asthma. At some point, occasionally as the initial presenting event as with Mark, sensitisation to aspirin or NSAIDs appears. The asthma and chronic sinusitis worsen over time, even with NSAID avoidance.4 In addition, these patients are more likely to have emergency department visits and hospitalisations, compared with those patients with asthma but not a diagnosis of AERD.5 Tolerance to daily low-dose aspirin does not preclude a patient having AERD.6
The reaction to NSAIDs in these patients is acquired and ‘pseudoallergic’, meaning it is not mediated by immunoglobulin E (IgE). Although the precise mechanism is not established, it is believed that affected patients have acquired alterations in the arachidonic acid metabolic pathway, which is the biochemical pathway affected by COX-1 inhibitors, resulting in an imbalance between proinflammatory and anti-inflammatory mediators.7-9 This imbalance is further increased on exposure to COX-1 inhibitors.
Diagnosis
The diagnosis of AERD is usually a clinical one based on the symptom triad of asthma and nasal polyps plus a linked respiratory reaction to the ingestion of an NSAID. Asthma with a normal CT scan of the sinuses and, conversely, nasal polyps and pansinusitis on imaging without asthma, make the diagnosis of AERD unlikely.10
In patients with both asthma and opacified sinuses on imaging who experience respiratory symptoms within 90 minutes of ingestion of an NSAID on one occasion, there is an 80% likelihood of a positive oral aspirin challenge result. This rises to 89% if the reaction has occurred on two or more occasions, and to 100% if NSAID ingestion provoked severe respiratory symptoms requiring hospital admission.10 It should be noted, however, that in patients with asthma and sinus disease in the absence of exposure to NSAIDs, less than half (42%) will have a positive oral aspirin challenge result.11
When a patient’s history of a possible reaction to NSAIDs is not clear, a formal aspirin challenge that induces recognisable respiratory symptoms and changes in lung function is the current standard for diagnosing AERD. As this is a provocative test that can induce severe bronchoconstriction, to undergo the test the patient must have well-controlled asthma, with an FEV1 of more than 1.5 L and 70% predicted or greater,12 and the test must be carried out in a hospital or clinic with a team experienced with the test. A recently proposed alternative diagnostic test uses low-dose aspirin (40 mg) and measurement of exhaled nitric oxide (FeNO) levels one hour later.13 Data showed that FeNO levels decreased significantly from baseline (mean, 19%) in patients with AERD, but increased or were stable in patients with aspirin-tolerant asthma.13 A sensitivity of 90% and specificity of 100% were reported.13
Additional characteristics make the diagnosis of AERD more likely. Up to 70% of patients report sensitivity to red wine and other alcoholic beverages14 or foods that have high levels of natural salicylates, such as dried apricots, as is the case with Mark. Complete anosmia associated with nasal polyps and the rapid regrowth of nasal polyps after first sinus or polyp resection are also suggestive of a diagnosis of AERD.
Management
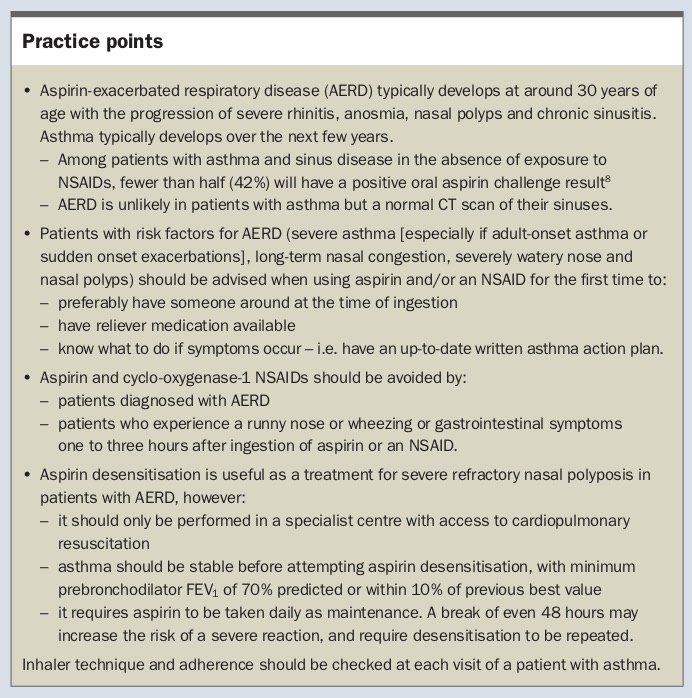
The medical management of a patient with AERD follows stepwise guideline-based management for patients with asthma, and guideline-based management for chronic rhinosinusitis with nasal polyposis. Important practice points are summarised in the Box. Add-on leukotriene receptor antagonists (such as montelukast) may provide additional clinical benefit to inhaled therapies by addressing the underlying dysregulation of leukotriene production.15
{kind=link}
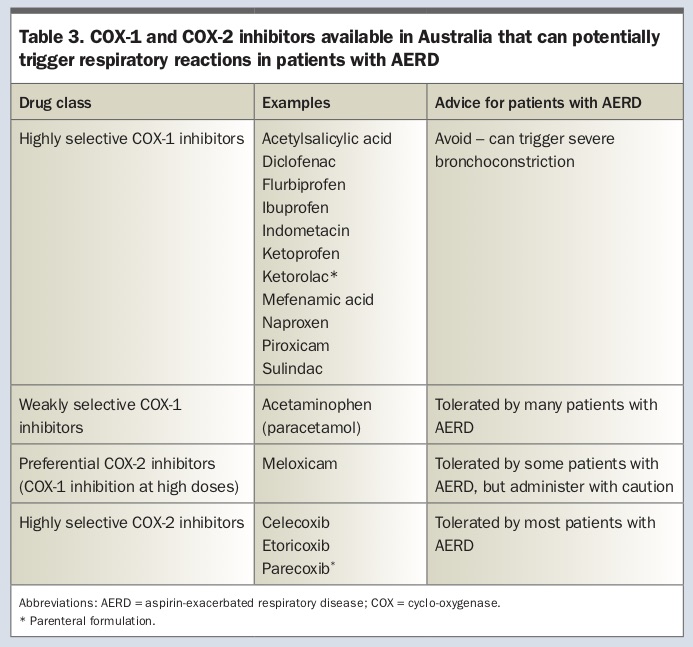
Importantly, patients with confirmed AERD should avoid all NSAIDs that inhibit COX-1 unless they have been desensitised to aspirin. Most COX-1 inhibitors are sold as tablets or capsules for oral consumption, except for ketorolac trometamol, which is available in tablet form and in solution for intravenous, intranasal and intramuscular injection. In patients with AERD, ketorolac trometamol in intravenous form produces a reaction in about 15 minutes.16 Acetaminophen is a weak inhibitor of COX-1, and induces a mild respiratory reaction in a minority of patients at high doses (1000 mg to 1500 mg).17 Specific COX-2 inhibitors do not cause respiratory reactions in patients with AERD18 and can be taken safely as alternatives for pain relief (Table 3).
{kind=link}
Surgical treatment of nasal polyps with debulking of the inflammatory nidus (eosinophilic polyps) and functional endoscopic sinus surgery to provide ventilation of the sinuses and facilitate intranasal drug delivery are usually required.19 As polyps recur rapidly, aspirin desensitisation may have a role to play shortly after sinus surgery to reduce the need for further surgery, which was the reason Mark was referred for desensitisation.
Aspirin desensitisation and treatment with aspirin
Aspirin desensitisation is a process of inducing tolerance to all NSAIDs, but requires the patient to continue daily use of low-dose aspirin to maintain the desensitised state.
Aspirin desensitisation and daily aspirin treatment is regarded as an important treatment option in patients with AERD, as their asthma is usually inadequately controlled with standard medical and surgical therapies. Aspirin desensitisation must only be attempted in a specialised centre with cardiopulmonary resuscitation capabilities because of the risk of severe reactions.
The optimal daily dose of aspirin after desensitisation is not known, with doses between 325 mg and 1300 mg reported as beneficial.12 Aspirin has been shown to slow the rate of polyp formation in patients with nasal polyposis refractory to surgery and topical corticosteroid therapy.20,21 There is evidence that the higher maintenance dose of 650 mg twice daily may also control airways disease in patients with AERD.22,23 Additional indications for desensitisation may include the need for antiplatelet therapy in patients with risk factors for or established cardiovascular disease, or the need for NSAIDs in treating chronic inflammatory disorders.
An individualised approach is required to determine the likelihood the patient will benefit from and strictly adhere to the maintenance treatment with daily aspirin. If aspirin is discontinued for longer than 48 to 96 hours, the patient should not resume taking aspirin, but rather be referred for repeat desensitisation. The risk of gastrointestinal toxicity should also be assessed and reviewed with the patient before commencing desensitisation. Of importance, desensitisation is an extension of the aspirin challenge and is a provocative test likely to induce symptoms of wheezing and bronchospasm, thus the patient’s asthma should be well controlled at the time of the procedure.
Biologic agents
Biologic agents may be a potential add-on treatment for patients with AERD who cannot tolerate either aspirin desensitisation or subsequent daily aspirin therapy,22 or who do not derive sufficient benefit from it. Both omalizumab (anti-IgE monoclonal antibody) and mepolizumab (anti-IL-5 monoclonal antibody) have been studied in the treatment of patients with AERD. A small randomised controlled trial of omalizumab in patients with nasal polyps and asthma (of whom half had AERD) showed improvement in both endoscopic polyp scores as well as nasal and asthma symptoms.24
Two small randomised trials involving mepolizumab looked at patients with severe recurrent nasal polyposis refractory to corticosteroid therapy, without stratification based on aspirin tolerance. They showed improvement in nasal polyposis scores and CT size scores,25 as well as a reduced need for nasal polyp surgery and improved sinonasal outcome test (SNOT)-22 scores.26 SNOT-22 is a validated questionnaire quantifying upper respiratory tract symptoms, with a change of 8.9 or more representing the minimally important difference.27 An additional retrospective study of 14 patients with severe asthma and AERD who received at least three doses of mepolizumab has been reported.28 Half (seven) of these patients were on oral glucocorticoids at the time of initiation. After three or more doses the mean absolute eosinophil count decreased significantly and the mean SNOT-22 score decreased by a clinically significant 17.7 points. In addition, overall asthma control test (ACT) mean scores increased by 5.1 (the minimally important difference being three)29 and five of the seven patients on oral glucocorticoids were able to reduce their doses. This indicates that mepolizumab may be useful to treat both the upper and lower respiratory tract symptoms of patients with AERD.
Mark’s progress
Mark was provided with information about his asthma, including the risks and potential impact on his family of life-threatening exacerbations with uncontrolled asthma, the need for regular preventer therapy with corticosteroids for both his asthma and his nasal polyposis, as well as extensive inhaler and nasal medicine technique education. Given the severity of his asthma, he was prescribed budesonide/formoterol maintenance therapy at high dose for the first month, 400/12 mcg two inhalations twice daily via a dry powder inhaler. Aspirin desensitisation was postponed indefinitely owing to both his inadequately controlled asthma and his low medication adherence.
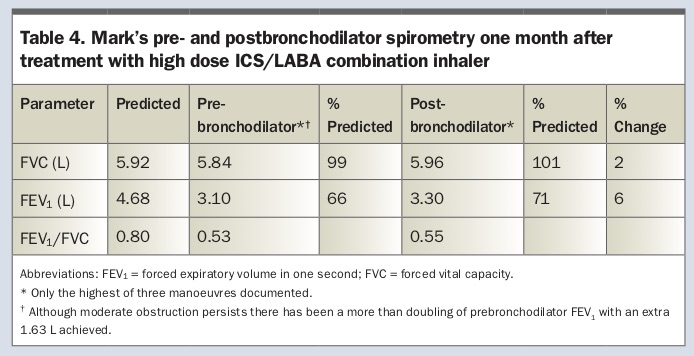
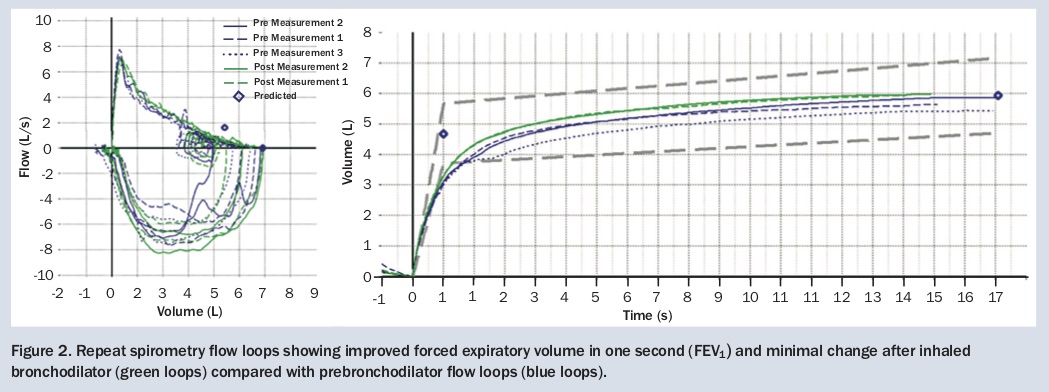
He returned a month later and, somewhat surprisingly given the substantial barriers to adherence expressed at the first visit, reported that he had taken his combination inhaler regularly. He had experienced minimal symptoms beyond the first few days of therapy and had not needed his reliever in the past month. He could run around with his children without becoming breathless and had noticed an improvement in his rhinorrhoea and post-nasal drip. His FEV1 (Table 4, Figure 2) had doubled compared with one month earlier (FEV1, 3.10 L; 66% predicted) and increased by a further 7% (to 3.30 L; 71% predicted) after salbutamol administration. His FVC was now normal at 5.84 L (99% predicted). He was switched to a moderate dose maintenance and reliever therapy (‘MART’) regimen, i.e. budesonide/formoterol (eformoterol) 200/6 mcg two puffs twice daily and one puff as needed for relief of symptoms. Use of this regimen provides the greatest reduction in risk of asthma exacerbations and would ensure that, even if he was poorly adherent, he would be getting some preventer medication and would not be exposed to the risks of treatment with only short-acting beta-2 agonists.30
{kind=link}
{kind=link}
Despite Mark’s substantial improvement, his airflow limitation is still too severe for aspirin desensitisation to be considered. Stabilisation of his airway hyper-responsiveness is likely to take at least several more months of regular daily treatment. If Mark’s asthma or nasal symptoms again become uncontrolled, or if he continues to have exacerbations despite good adherence with high dose combination inhaler therapy, he could be given a trial of add-on leukotriene receptor antagonist and/or considered for eligibility for a biologic therapy for severe asthma. RMT